
4150 Technology Way, Suite 300 ● Carson City, Nevada 89706
775-684-4200 ● Fax 775-687-7570 ● dpbh.nv.gov
Page 1 of 1
Steve Sisolak
Governor
Richard Whitley, MS
Director
DEPARTMENT OF
HEALTH AND HUMAN SERVICES
DIVISION OF PUBLIC AND BEHAVIORAL HEALTH
Helping people. It’s who we are and what we do.
Lisa Sherych
Administrator
Ihsan Azzam,
Ph.D., M.D.
Chief Medical Officer
__________________________________________________________________________________________________
December 28, 2022
Brenda Erdoes
Director, Legislative Counsel Bureau
401 South Carson Street
Carson City, Nevada 89701
Dear Director Erdoes,
Please find attached for your review the 2020-2021 Maternal Mortality Review Committee Legislative Report due to the
Director of the Legislative Counsel Bureau per Nevada Revised Statutes 442.767.
Thank you for your time and consideration.
Sincerely,
Richard Whitley, MS
Director, Department of Health and Human Services
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 1
Maternal Mortality and
Severe Maternal Morbidity
Nevada, 2020-2021
December 2022
Office of Analytics
and
Maternal, Child, and Adolescent Health Section,
Division of Public and Behavioral Health
Department of Health and Human Services
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 2
Acknowledgements
Report Prepared by:
Praseetha Balakrishnan, MS
Biostatistician II
Office of Analytics
Nevada Department of Health and Human Services
Editing, Review, and Comments:
Jie Zhang, MS
Management Analyst III
Office of Analytics
Nevada Department of Health and Human Services
Jen Thompson
Health Program Manager II
Office of Analytics
Nevada Department of Health and Human Services
Alexia Benshoof, MS
Health Bureau Chief
Office of Analytics
Nevada Department of Health and Human Services
Kyra Morgan, MS
Chief Biostatistician
Office of Analytics
Nevada Department of Health and Human Services
Vickie Ives, MA
Deputy Bureau Chief
Bureau of Child, Family and Community Wellness
Division of Public and Behavioral Health
Nevada Department of Health and Human Services
Tami Conn, MPH
Section Manager
Maternal, Child, and Adolescent Health
Division of Public and Behavioral Health
Nevada Department of Health and Human Services
For Additional Information Contact:
For data-related questions: For maternal health-related questions:
Office of Analytics Maternal, Child and Adolescent Health
Nevada Department of Health and Human Services Bureau of Child, Family and Community Wellness
data@dhhs.nv.gov Division of Public and Behavioral Health
Vickie Ives, MA: vives@health.nv.gov
Tami Conn, MPH: tconn@health.nv.gov
Recommended Citation:
Office of Analytics. Department of Health and Human Services. Maternal Mortality and Severe Maternal Morbidity
Nevada, 2020-2021. Carson City, Nevada. December 2022.
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 3
Table of Contents
Acknowledgements ...................................................................................................................................................... 2
Table of Contents .......................................................................................................................................................... 3
Executive Summary ...................................................................................................................................................... 5
Key Recommendation Themes and Priorities of the Maternal Mortality Review Committee and the Advisory
Committee of the Office of Minority Health and Equity .............................................................................................. 5
Data and Equity Statement ........................................................................................................................................... 7
Background ................................................................................................................................................................... 7
Maternal Mortality Data ............................................................................................................................................... 8
Definitions Associated with Maternal Mortality ...................................................................................................... 8
National Maternal Mortality Statistics ..................................................................................................................... 9
Pregnancy-Associated Death (PAD) ........................................................................................................................ 11
Methodology ...................................................................................................................................................... 11
General Statistics ................................................................................................................................................ 14
Maternal Demographics ..................................................................................................................................... 15
Underlying Causes of Pregnancy-Associated Deaths.......................................................................................... 20
Pregnancy-Related Death (PRD) ............................................................................................................................. 24
Methodology ...................................................................................................................................................... 24
General Statistics ................................................................................................................................................ 24
Maternal Demographics ..................................................................................................................................... 25
Underlying Causes of Pregnancy-Related Deaths ............................................................................................... 30
Maternal Deaths ..................................................................................................................................................... 32
Methodology ...................................................................................................................................................... 32
General Statistics ................................................................................................................................................ 32
Maternal Demographics ..................................................................................................................................... 33
Severe Maternal Morbidity (SMM) Data .................................................................................................................... 34
Definition ................................................................................................................................................................ 34
National Severe Maternal Mortality Statistics........................................................................................................ 34
Methodology .......................................................................................................................................................... 35
Data Sources ....................................................................................................................................................... 35
Identification of Severe Maternal Morbidity ....................................................................................................... 35
Analysis ............................................................................................................................................................... 36
General Statistics ................................................................................................................................................ 37
Indicators Associated with SMM ........................................................................................................................ 37
Maternal Demographics ..................................................................................................................................... 39
Data Summary ............................................................................................................................................................ 43
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 4
Maternal Mortality Reviewed by the MMRC ............................................................................................................. 44
MMRC Recommendations .......................................................................................................................................... 45
General MMRC Member MM/SMM Recommendations and Prevention .............................................................. 50
Advisory Committee of the Office of Minority Health and Equity Recommendations .......................................... 50
Advisory Committee of the Office of Minority Health and Equity Members ......................................................... 51
Maternal Mortality Review Committee Members ................................................................................................. 51
MMRC Support Staff and Other Acknowledgements ............................................................................................. 52
Appendix ..................................................................................................................................................................... 53

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 5
Executive Summary
The death of a person during pregnancy, at delivery, or soon after delivery is a tragedy for their family and for
society. Sadly, approximately 700 people die each year in the United States because of pregnancy or delivery
complications.
1
From 2018-2020, Nevada had 20 pregnancy-related deaths.
2
Several Nevada mortality statistics are highlighted below, including:
▪ The state maternal mortality rate from 2018-2020 (19.2 per 100,000 live births)
2
is higher than the
Healthy People 2030 objective of 15.7.
3
▪ Black, non-Hispanic Nevadans had mortality rates that were 4.3 times higher than rates for White, non-
Hispanic Nevadans (80.7 vs. 18.7) and 5.2 times higher than Hispanic Nevadans (15.4) from 2017 through
2018.
▪ In the years 2020 to 2021, American Indian/Alaska Native (AI/AN), non-Hispanic Nevadans had the highest
pregnancy-associated death ratio at 501.7 per 100,000 live births followed by Black, non-Hispanic
Nevadans at 199.4 per 100,000 live births.
▪ The rate in Clark County (35.5) was 3.7 times higher than Washoe County (9.5).
▪ The rate was highest among individuals 35-39 years of age (71.9) and was 5.4 times higher than those
who are 20-24 years of age (13.4).
▪ Distribution of 2020 and 2021 pregnancy associated deaths occurred during pregnancy 17.7%, within 42
days postpartum 24%, and between 43 and 365 days postpartum 58.2%.
One major risk factor for maternal mortality is severe maternal morbidity (SMM). SMM refers to unexpected
outcomes of labor and delivery that result in major consequences to health.
5,6
SMM increases medical costs,
lengthens hospitalization stays,
5
and increases the risk of postpartum maternal morbidity and mortality,
particularly among pregnant person with hypertensive disorders.
7
SMM rates have been increasing nationally,
5
including in Nevada.
▪ Among 60,813 delivery hospitalizations from 2020 through 20121, 414 were SMM cases (excluding blood
transfusions), for a SMM rate of 68.1 per 10,000 delivery hospitalizations.
o When blood transfusions are added, the rate increases to 192.1 per 10,000 with 1,168 cases.
▪ From 2016 through 2021, SMM rates in Nevada increased from 126.5 to 205.0 per 10,000 delivery
hospitalizations with a total of 618 cases (including blood transfusions).
▪ Among Racial disparities in SMM exist:
o The SMM rate for Black, non-Hispanic (282.2) and AI/AN, non-Hispanic (277.8) individuals were
both approximately 1.7 times higher than the rate for White, non-Hispanic individuals (159.5),
even though these two groups only accounted for 21% and 1% of all SMM cases, respectively.
Key Recommendation Themes and Priorities of the Maternal
Mortality Review Committee and the Advisory Committee of
the Office of Minority Health and Equity
The Maternal Mortality Review Committee (MMRC) creates recommendations based on their review of deaths
that occur during or within a year of pregnancy in Nevada and their case-based recommendations and relevant
1
Centers for Disease Control and Prevention. Preventing Pregnancy Related Deaths. https://www.cdc.gov/reproductivehealth/maternal-mortality/preventing-pregnancy-related-deaths.html. Accessed
November 14, 2022.
2
National Center for Health Statistics. Maternal deaths and mortality rates: Each state, the District of Columbia, United States, 2018‐2020. https://www.cdc.gov/nchs/maternal-mortality/mmr-2018-2020-state-
data.pdf . Accessed December 18, 2022.
3
Pregnancy and Childbirth. Healthy People. https://health.gov/healthypeople/objectives-and-data/browse-objectives/pregnancy-and-childbirth. Accessed December 1, 2022.
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 6
statewide maternal mortality (MM) and severe maternal morbidity (SMM) data are provided to the Advisory
Committee of the Office of Minority Health and Equity which was added as a collaborator in 2021 as amended by
Nevada Revised Statutes 442.767 and which contributes recommendations. All recommendations are provided
later in the report, but some identified themes and priorities are highlighted below. These recommendations
include making improvements to mental health care, Medicaid coverage, transportation access, law enforcement
processes, increasing maternal health education, childcare access, and access to certain clinical services. The
following were identified as priority recommendations by the MMRC; the Advisory Committee of the Office of
Minority Health and Equity recommendations highlighted the importance of transportation and primary care
access, as well as the importance of the psychiatry rotation during residency MMRC recommendation:
• State of Nevada agencies and programs such as the Department of Health and Human Services, Division
of Public and Behavioral Health, and Behavioral Health and Wellness Program, as well as groups such as
the Perinatal Health Initiative, should develop a focused campaign and dedicate funding for
methamphetamine use in pregnancy reduction.
• State of Nevada agencies and programs should mandate priority access to mental health and medication
assisted substance use treatment for pregnant persons by July 1, 2025.
• Division of Child and Family Services, Department of Education, Nevada Part C and Early Intervention
Services programs should develop and implement early childhood intervention and trauma therapy for
impacted children by July 1, 2024.
• State Medicaid (Division of Health Care Financing and Policy) should receive funding from the State such
as a legislative appropriation to expand postpartum coverage in Nevada to 12 months to allow access to
behavioral health care and medical care by July 1, 2024.
• Medicaid policy and reimbursement changes for behavioral health care treatment should be allowed and
incentivized to encourage it to be performed within medical offices with equal Medicaid reimbursement
for medical and behavioral health services by the end of 2024.
• Institutions and hospitals should standardize response and reporting of abnormal perinatal vital signs and
severe pain to include not only pain treatment but prompt evaluation of the cause of acute pain and
presence of protocols to do so be part of licensing and certification processes for Health Care Quality and
Compliance, Division of Public and Behavioral Health by July 1, 2024.
• State of Nevada agencies and programs such as Nevada State Medicaid should improve availability and
use of perinatal case coordinators and improve patient communication, with Nevada State Medicaid to
receive funding, including but not limited to legislative appropriations to expand existing programs or
create new ones to improve perinatal health outcomes by December 31, 2024.
• Education by state medical professional associations by July 1, 2024, to prevent failure to recognize the
impact of obesity as a risk factor for poor perinatal outcomes.
Selected MM and SMM Prevention Efforts in Nevada are highlighted below:
• Establishment of a Nevada MMRC
• Alliance for Innovation in Maternal Health (AIM) patient safety bundle on hypertension in pregnancy
implementation. Nevada AIM launched the hypertension bundle in Fall 2022 and out of the 18 birthing
facilities in Nevada, the following are Nevada AIM-participants:
o Henderson Hospital
o Humboldt General Hospital
o Renown Regional Medical Center
o South Lyon Medical Center (Not a birthing facility, but participating in AIM)
o Summerlin Hospital
o Banner Churchill Hospital
o Centennial Hills Hospital
o Spring Valley
o Sunrise Hospital
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 7
o Dignity Health St. Rose San Martin Hospital
• Pregnancy Risk Assessment Monitoring System data collection and surveillance
• University of Nevada, Las Vegas, School of Nursing, Perinatal Regionalization Program
• Hear Her Campaign and maternal warning signs education efforts statewide
Data and Equity Statement
Demographic language may differ throughout this report depending on the sources from which data were
retrieved. To report the data accurately, variables such as race, ethnicity and sex are described in the data as they
were in the source data. Every effort has been made to be inclusive and equitable across every demographic to
provide a fair and accurate representation of the people of Nevada. We recognize the terms female and woman
do not include all birthing people but used descriptors as presented in source data, such as when referring to
rates per 100,000 women of reproductive age.
Background
The Nevada Maternal Mortality Review Committee was established per Nevada Revised Statutes (NRS) 442.764 in
2019, convening for the first time in 2020. The committee reviews all pregnancy-associated deaths in Nevada
(encompassing all deaths of Nevadans while pregnant or within one year of the end of pregnancy, due to any cause)
and develops recommendations to prevent future deaths. NRS 442.767 states that the Department of Health and
Human Services shall compile and publish a biennial report on or before December 31 of each even-numbered year
consisting of data, a summary of disparities, plans for corrective action, and policy and legislative recommendations
concerning maternal mortality and severe maternal morbidity in this State. This report will cover the years 2020
through 2021; these are the most recent two years for which complete, final data is available.
Maternal Mortality
Maternal mortality is defined as deaths due to complications from pregnancy or childbirth. This report provides
insight into demographic characteristics, cause of death, and drug overdose deaths associated with pregnancy‐
associated deaths from January 2020 to December 2021. This report also provides data on pregnancy-related
deaths from Pregnancy Maternal Surveillance System (PMSS) during 2012 through 2018. PMSS is a national
surveillance program conducted by the Centers for Disease Control and Prevention (CDC) to understand better the
risk factors for and causes of pregnancy‐related deaths in the United States. The Nevada Department of Health and
Human Services Office of Analytics annually provides a list of pregnancy‐associated deaths to the CDC.
1
Medically
trained epidemiologists at the CDC review and analyze the cases provided, determine which cases meet the CDC’s
definition of pregnancy‐related mortality, and send a list of cases back to the Office of Analytics. At the time of this
report, 2018 data was the latest year available which is included in this report. For more information on PMSS,
please visit CDC PMSS.
Severe Maternal Morbidity
Maternal morbidity is a continuum from mild adverse effects to life‐threatening events or death.
2
Severe Maternal
Morbidity (SMM) refers to conditions and diagnoses which indicate potentially life-threatening maternal
complications. SMM includes unexpected outcomes of labor and delivery resulting in significant short‐ or long‐term
consequences to health.
3
SMM relates to higher risks of adverse pregnancy outcomes like preterm birth and infant
1
Nevada Legislature website.
https://www.leg.state.nv.us/nrs/nrs-442.html#NRS442Sec767
2
Severe Maternal Morbidity, New York City, 2008‐2012. https://www1.nyc.gov/assets/doh/downloads/pdf/data/maternal‐morbidity‐report‐08‐12.pdf
3
American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine, Kilpatrick SK, Ecker JL. Severe maternal morbidity: screening and review. Am J Obstet
Gynecol. 2016;215(3): B17–B22.
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 8
death. SMM is associated with a high rate of preventability. SMM can be considered a near miss for maternal
mortality because, without identification and treatment, the conditions would lead to maternal death in some
cases. Identifying SMM is important for preventing injuries leading to mortality and highlighting opportunities to
avoid repeat injuries. This reports highlights Nevada disparity data on severe maternal morbidity across race,
ethnicity, geography, insurance status, education, age, as well as prenatal and delivery characteristics such as
prenatal care initiation, adequacy of prenatal care, parity, method of delivery, plurality, and chronic disease.
This report is divided into a section on MM, SMM, and MM prevention recommendations of the Nevada Maternal
Mortality Review Committee and the Advisory Committee of the Office of Minority Health and Equity per NRS
442.767.
Maternal Mortality Data
As noted previously, maternal mortality is defined as deaths due to complications from pregnancy or childbirth.
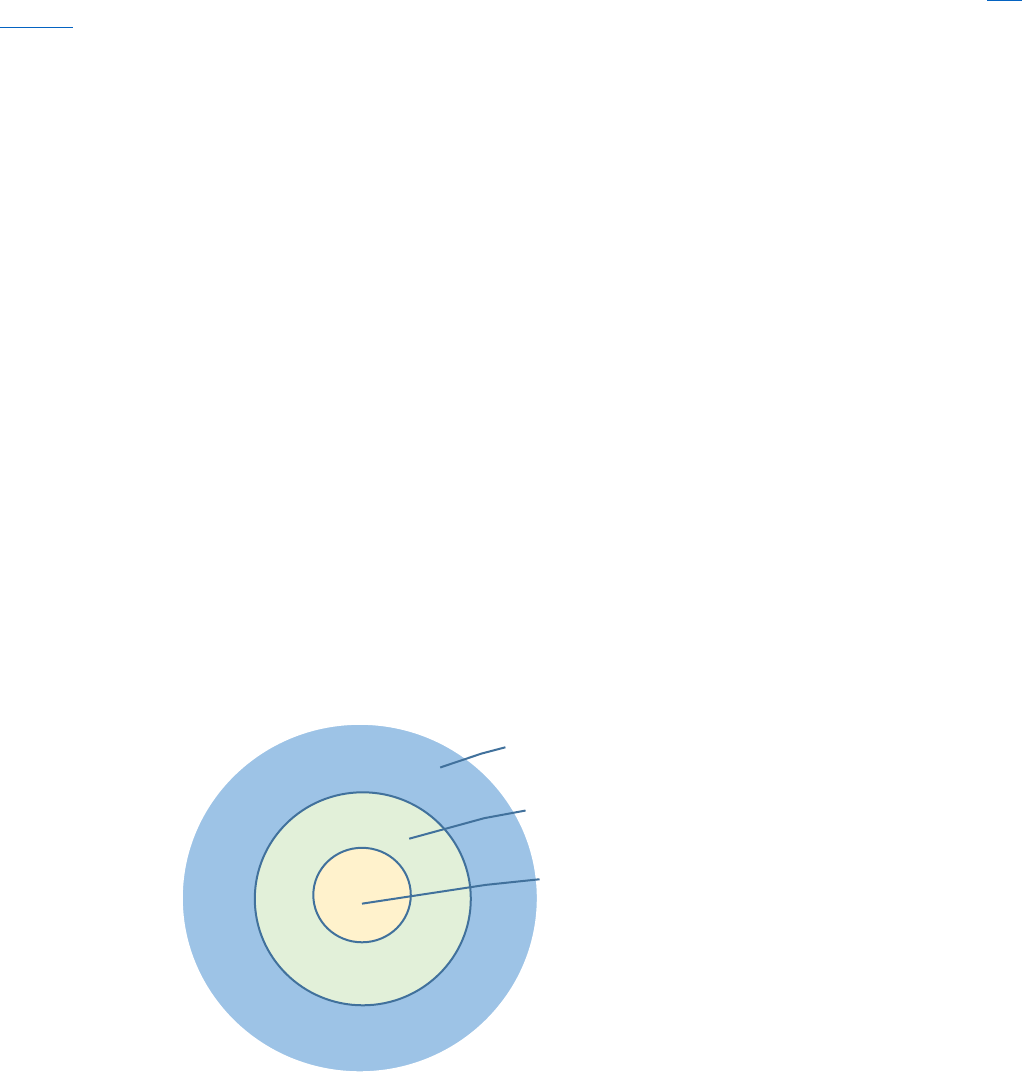
There are three terms or definitions related to maternal mortality and they are described below and shown in
Figure 1.
Definitions Associated with Maternal Mortality
Pregnancy-Associated Death (PAD) is the death of a person while pregnant or within one year of the termination
of pregnancy, regardless of the cause. Pregnancy-associated death ratio is the number of pregnancy-associated
deaths per 100,000 live births.
Pregnancy-Related Death (PRD) is the death of a person during pregnancy or within one year of the end of
pregnancy, from a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an
unrelated condition by the physiologic effects of pregnancy. Pregnancy-related death ratio is the number of
pregnancy-related deaths per 100,000 live births.
Maternal Death is the death of a person while pregnant or within 42 days of the termination of pregnancy,
regardless of the duration and site of pregnancy, from any cause related to or aggravated by the pregnancy or its
management, but not from accidental or incidental causes.
Figure 1. Relationship Among Three Parts of Maternal Mortality – Pregnancy-Associated Deaths, Pregnancy-Related
Deaths, and Maternal Deaths
Maternal Deaths
Pregnancy-Related Deaths
Pregnancy-Associated Deaths
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 9
The Maternal Mortality section of this report will explore Pregnancy-Associated Deaths, then Pregnancy-Related
Deaths, and finally Maternal Deaths.
National Maternal Mortality Statistics
The most recent national statistics on maternal mortality are available through 2020. The United States has the
highest maternal mortality ratio of industrialized countries, and this ratio is increasing
5
. Across the United States in
2020, 861 maternal deaths occurred during delivery or within 42 days of delivery. The maternal mortality rate in
2020 was 23.8 deaths per 100,000 live births, an increase from 2019 (20.1 deaths per 100,000 live births) and 2018
(17.4 deaths per 100,000 live births).
6,
7
addition, in 2020, the United States had the highest maternal mortality rate
among 11 developed countries.
8
Many cases of maternal mortality and morbidity are preventable.
9
Many of the
strategies for preventing maternal mortality also reduce maternal morbidity, and timely and appropriate prenatal,
delivery, and postpartum care is associated with better maternal health outcomes.
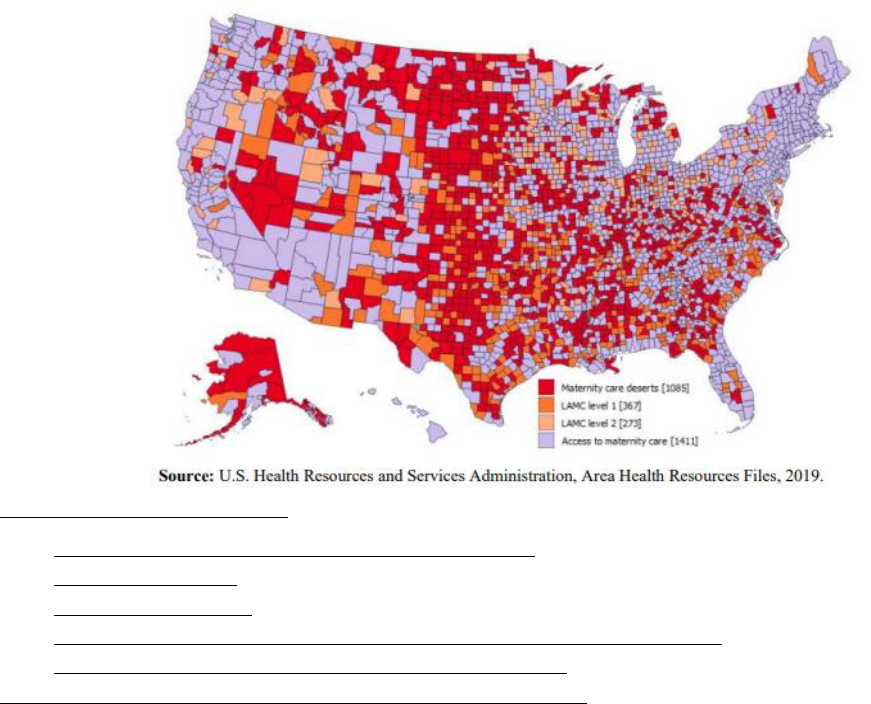
The below map (Figure 2) shows the locations of maternity care deserts, defined as counties with no hospital
offering obstetric care and no obstetric providers. It also presents limited access to maternity care (LAMC) counties,
defined as counties with fewer than two hospitals offering obstetric care and fewer than 60 obstetric/gynecologic
(OB-GYN) providers per 10,000 births. The counties are separated into LAMC level 1, where 10% or more of those
ages 18-64 lack health insurance, and LAMC level 2, where less than 10% of those ages 18-64 lack health insurance.
Only 6% of OB-GYNs are in rural areas and the ratio of OB-GYNs per 10,000 women is lower in nonmetropolitan
areas than in metropolitan areas.
10 ,12
Figure 2. Access to Maternity Care in U.S. Counties, 2016
5
2022 National Healthcare Quality and Disparities Report
https://www.ahrq.gov/sites/default/files/wysiwyg/research/findings/nhqrdr/2022qdr.pdf#page=9
6
Hoyert DL. Maternal mortality rates in the United States, 2019. NCHS Health E-Stats. 2021.
https://doi.org/10.15620/cdc:103855. Accessed October 3, 2022
7
Hoyert DL. Maternal mortality rates in the United States, 2020. NCHS Health E-Stats. 2022.
https://dx.doi.org/10.15620/cdc:113967. Accessed October 3, 2022.
8
Maternal Mortality and Maternity Care in the United States Compared to 10 Other Developed Countries. Issue Brief. New York, NY: The Commonwealth Fund; November 2020.
https://www.commonwealthfund.org/publications/issue-briefs/2020/nov/maternal-mortality-maternity-care-us-compared-10-countries Accessed October 3, 2020.
9
Centers for Disease Control and Prevention. Preventing Pregnancy-Related Deaths. Last reviewed April 2022.
https://www.cdc.gov/reproductivehealth/maternal-mortality/preventing-pregnancy-related-deaths.html. Accessed October 3, 2022.
10
Health Disparities in Rural Women Committee Opinion Number 586. Washington, DC: American College of Obstetricians and Gynecologists; February 2014.
https://www.acog.org/clinical/clinical-guidance/committeeopinion/articles/2014/02/health-disparities-in-rural-women/ Accessed October 3, 2022.
12
Callaghan WM, Creanga AA, Kuklina EV. Severe Maternal Morbidity Among Delivery and Postpartum Hospitalizations in the United States. Obstetrics and Gynecology 2012; 120:1029‐36.
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 10
Large portions of rural Nevada are designated as maternity care deserts as shown in the map above which may
have an impact on maternal mortality and other maternal health outcomes.

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 11
Pregnancy-Associated Death (PAD)
Methodology
Data Sources
Web-Enabled Vital Records Registry Systems (WEVRRS)
Statewide births, deaths, and fetal deaths are collected by the Office of Vital Records in the Division of Public and
Behavioral Health. WEVRRS is a software utilized by physicians, registered nurses, midwives, informants or funeral
directors, and other individuals to collect and consolidate birth and death-related information.
Hospital Billing Data (Emergency Department Encounter and Hospital Inpatient Admissions)
The hospital billing data provides health billing data for emergency department encounters and inpatient
admissions for Nevada’s non-federal hospitals. NRS 449.485 mandates all hospitals in Nevada report discharge
information as prescribed by the Director of the Department of Health and Human Services. The data are collected
using a standard universal billing form. The data includes demographics such as age, gender, race/ethnicity, and
uses International Classification of Diseases-9-Clinical Modification (ICD-9-CM) diagnoses codes and International
Classification of Diseases-10-Clinical Modification (ICD-10-CM) diagnoses. ICD-10-CM diagnoses codes replaced ICD-
9-CM diagnoses codes in the last quarter of 2015. Therefore, data prior to last quarter in 2015 may not be directly
comparable to data thereafter. In addition, the data includes billed hospital charges, procedure codes, discharge
status, and external cause of injury codes. The billing information is for billed charges and not the actual payment
received by the hospital.
State Demographer Data
The Nevada State Demographer provides the Nevada population of women of reproductive age which is used in
calculating rates.
Identification of Pregnancy-Associated Deaths
The methodology is based on Reference Guide for Pregnancy-Associated Death Identification which was developed
by the Pregnancy-Associated Death Identification Workgroup, consisting of members from state departments of
health and the Centers for Disease Control and Prevention (CDC)
4
.
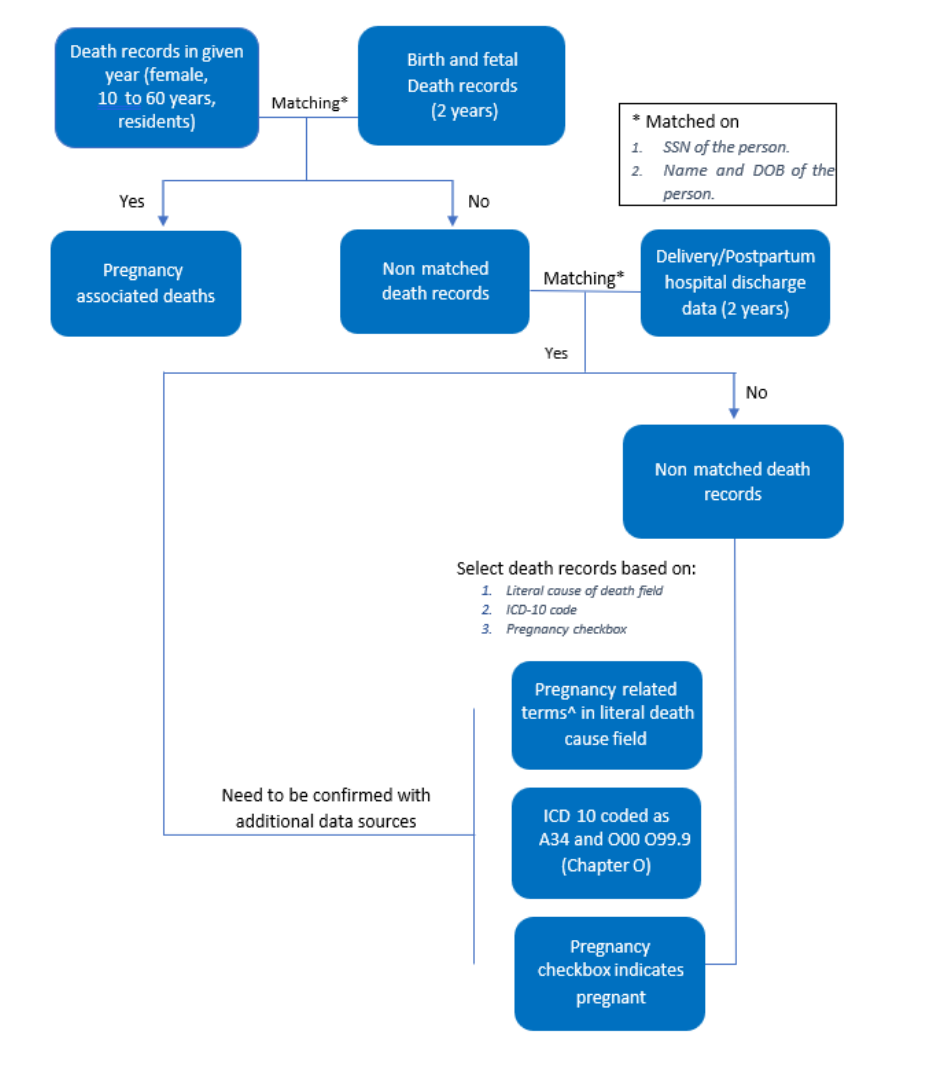
Identification by Vital and Hospital Discharge Records Linkages
A death data set is created for a given year for all Nevada female residents aged 10 to 60 years. Two data sets (birth
and fetal death records, delivery and postpartum emergency department encounter and hospital inpatient
admission records) are created for the same given calendar year and previous calendar year. Death records of
people aged 10 to 60 years are first linked with birth and fetal death records based on mother’s social security
number (SSN). Death records of people ages 10-60 years that are not linked using SSN are then matched to birth
and fetal death records using mother’s first name, mother’s last name, and mother’s date of birth. Non-matched
death records are then linked with delivery and postpartum emergency department encounter and hospital
inpatient admission records based on mother’s SSN, mother’s name, and date of birth. SAS software is used for the
linkages.
Identifying by Causes of Death Information
4
Centers for Disease Control and Prevention (CDC). “Reference Guide for Pregnancy-Associated Death Identification.”
https://reviewtoaction.org/sites/default/files/2022-08/Reference%20Guide%20for%20Pregnancy-Associated%20Death%20Identification.pdf
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 12
Some pregnancy-associated deaths, such as those occurred early during pregnancy, will not have birth or fetal death
records to link. In order to identify pregnancy-associated deaths among those death records, we select death
records of female aged 10 to 60 where the underlying causes of death were coded in A34 and O00-O99.9 (i.e. ICD-
10 codes related to pregnancy) and/or the literal death cause field contains any of the following pregnancy-related
terms: amniotic, chorioamnionitis, eclampsia, ectopic, intrauterine fetal demise, peripartum, peripartum
cardiomyopathy, placental, postpartum, pregnancy, pregnant, uterine hemorrhage, and uterine rupture. Selected
pregnancy-associated deaths should be confirmed with additional data sources to avoid misclassification. Examples
of additional confirmatory sources are provided in the section on Additional Data Sources.
Identifying by Pregnancy Checkboxes on the Death Records
Death records were also selected for females aged 10 to 60 where the pregnancy checkbox on the death record
was checked as: pregnant at time of death, not pregnant but pregnant within 42 days of death, or not pregnant but
pregnant 43 days to one year before death. Selected pregnancy-associated deaths should be confirmed with
additional data sources to avoid misclassification. Examples of additional confirmatory sources are provided in the
section on Additional Data Sources.
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 13
Figure 3. Flow Chart of Identifying Pregnancy-Associated Deaths
^ Pregnancy-related terms are amniotic, chorioamnionitis, eclampsia, ectopic, intrauterine fetal demise, peripartum,
peripartum cardiomyopathy, placental, postpartum, pregnancy, pregnant, uterine hemorrhage, and uterine
rupture.
Additional Data Sources
Additional data sources identified by the Pregnancy-Associated Death Identification Workgroup that can help
confirm pregnancy for deaths which do not link to vital records and hospital discharge records, but have pregnancy
indicated by causes of death information and/or pregnancy checkbox on the death record.
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 14
• Obituaries
• Social Media
• Media and News Reports
• Certifier Confirmation
• Autopsy Reports
Analysis
The analyses in the report are for pregnancy-associated deaths for Nevada residents only. Pregnancy-associated
death ratio is the number of pregnancy-associated deaths per 100,000 live births. The calculation for maternal
mortality ratio = (Number of resident maternal deaths/Number of resident live births) x 100,000. Pregnancy-related
death rate is the number of pregnancy-related deaths per 100,000 women of reproductive age. The calculation for
maternal mortality rate = (Number of resident maternal deaths/Number of resident women of reproductive age) x
100,000.
The linkages and analyses were performed by using SAS 9.4.
General Statistics
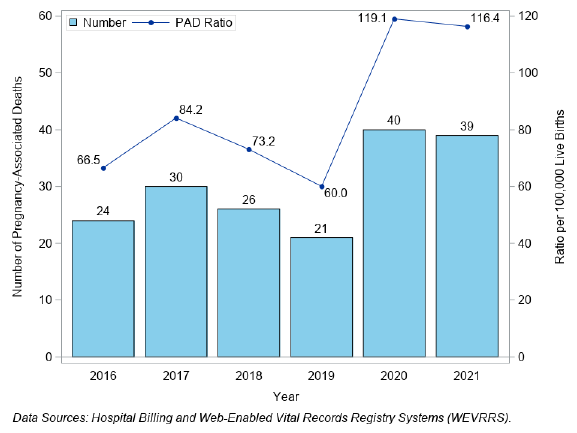
There were 180 pregnancy-associated deaths in Nevada from 2016 to 2021 (sum of counts by year in Figure 4).
There were total of 79 pregnancy-associated deaths from January 2020 to December 2021.
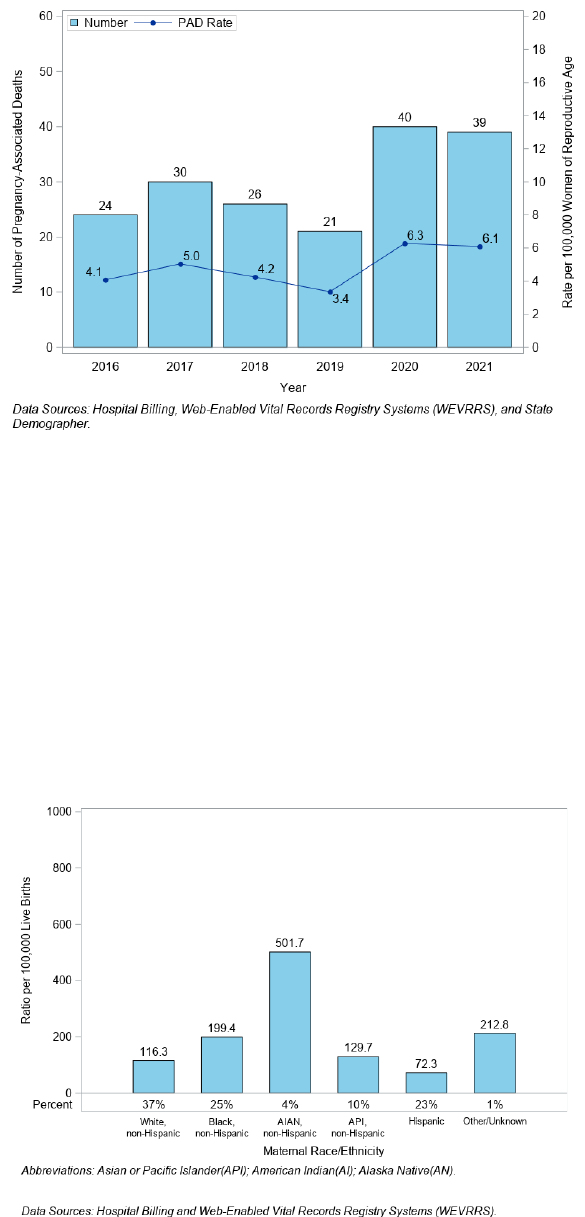
The highest ratio was in 2020, at 119.1 per 100,000 live births (Figure 4) and a rate of 6.3 per 100,000 women of
reproductive age (Figure 5).
Figure 4. Number of Pregnancy-Associated Deaths (PAD) and Death Ratio per 100,000 Live Births, Nevada, 2016-
2021
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 15
Figure 5. Number of Pregnancy-Associated Deaths (PAD) and Death Rate per 100,000 Women of Reproductive Age,
Nevada, 2016-2021
Maternal Demographics
A total of 79 Nevadans had a pregnancy-associated death during 2020 to 2021. By race and ethnicity, these
Nevadans who died were 37% White, non‐Hispanic, 25% Black, non‐Hispanic, 23% Hispanic, 10% Asian/Pacific
Islander (API), non‐Hispanic, 4% were American Indian/Alaska Native (AI/AN), non‐Hispanic.
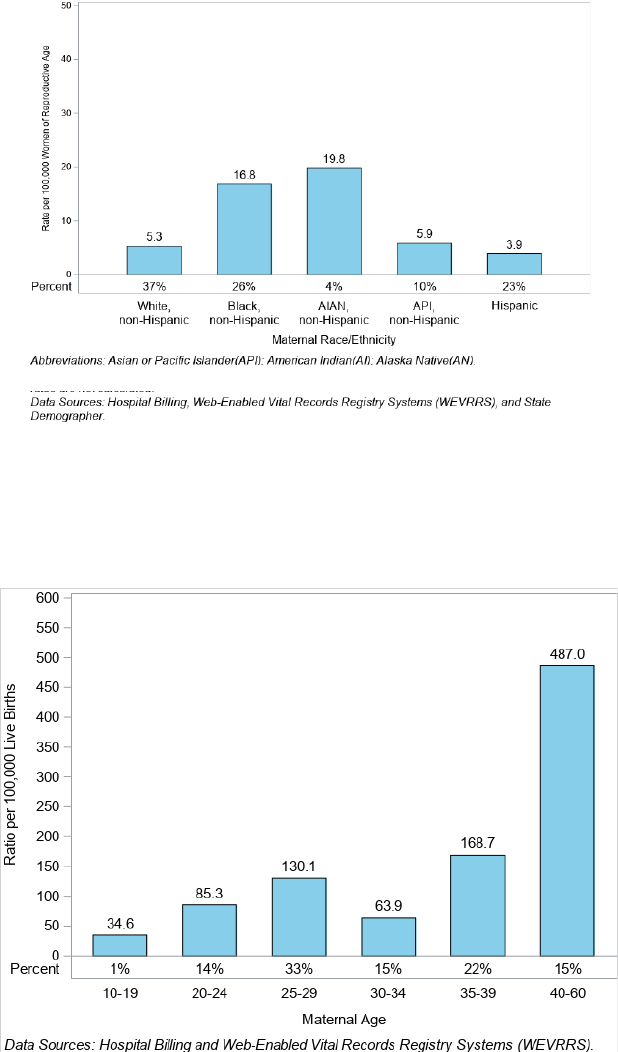
Figure 6 shows that AI/AN, non-Hispanic Nevadans had highest pregnancy-associated death ratio at 501.7 per
100,000 live births and accounted for 4% of the pregnancy-associated deaths. Excluding the Other/Unknown
category, Black, non-Hispanic Nevadans had the second highest ratio at 199.4 per 100,000 live births. Hispanic
Nevadans had the lowest death ratio at 72.3 per 100,000 live births, accounting for 23% of all pregnancy‐associated
deaths.
Figure 6. Pregnancy-Associated Death (PAD) Ratio and Percent by Maternal Race/Ethnicity, Nevada, 2020-2021
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 16
AI/AN, non‐Hispanic Nevadans had the highest death rate at 19.8 per 100,000 women of reproductive age (Figure
7).
Figure 7. Pregnancy-Associated Death (PAD) Rate and Percent by Race/Ethnicity, Nevada, 2020-2021
Nevadans aged 40+ had the highest pregnancy-associated death ratio at 487 per 100,000 live births, followed by
the 35 to 39 age group at a ratio of 168.7 per 100,000 live births (Figure 8). Nevadans aged 35 and older accounted
for a total of 37% of deaths.
Figure 8. Pregnancy-Associated Death (PAD) Ratio and Percent by Maternal Age, Nevada 2020-2021
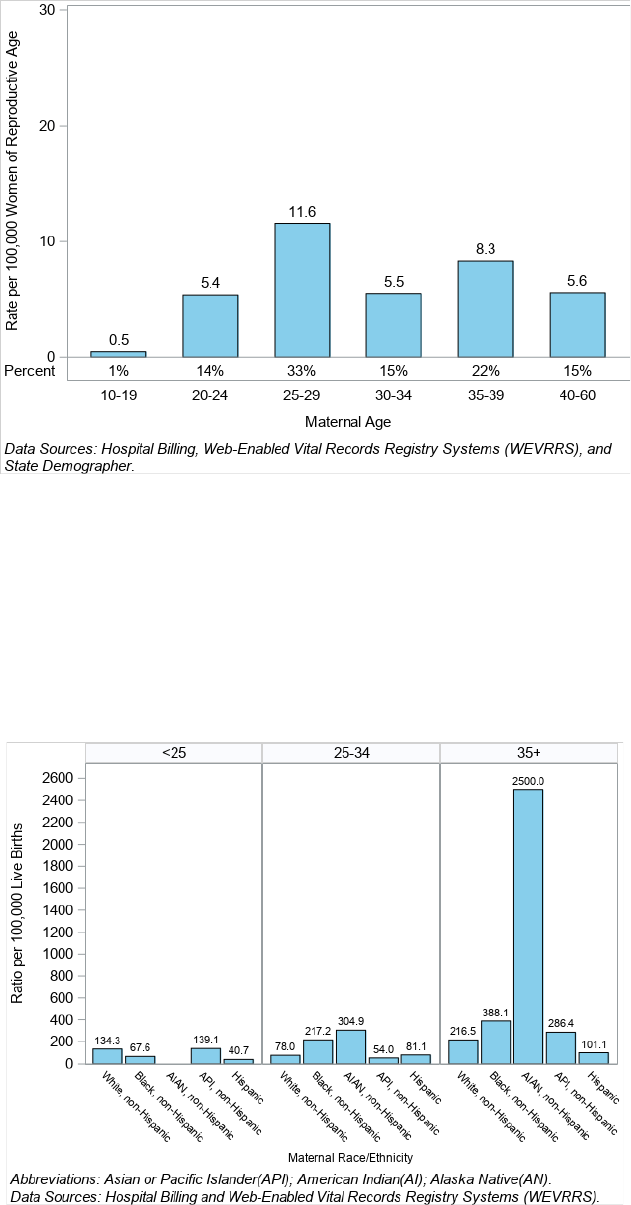
Nevadans aged 25 to 29 years had the highest pregnancy-associated death rate at 11.6 per 100,000 women of
reproductive age (Figure 9).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 17
Figure 9. Pregnancy-Associated Death (PAD) Rate and Percent by Maternal Age, Nevada 2020-2021
Figure 10 illustrates the pregnancy-associated death ratio for each race and ethnicity within the age groups of <25,
25 to 34, and 35 and older. For age group <25, Asian/Pacific Islander (API) Nevadans had the highest PAD ratio at
139.1 per 100,000 live births. For age group 35+, AI/AN, non-Hispanic Nevadans had the highest PAD ratio at 2500
per 100,000 live births, followed by Black, non-Hispanic at 388.1 per 100,000 live births; there was no count for
American Indian/Alaska Native (AI/AN) for age group <25.
Figure 10. Pregnancy-Associated Death (PAD) Ratio by Maternal Age and Race/Ethnicity, Nevada 2020-2021
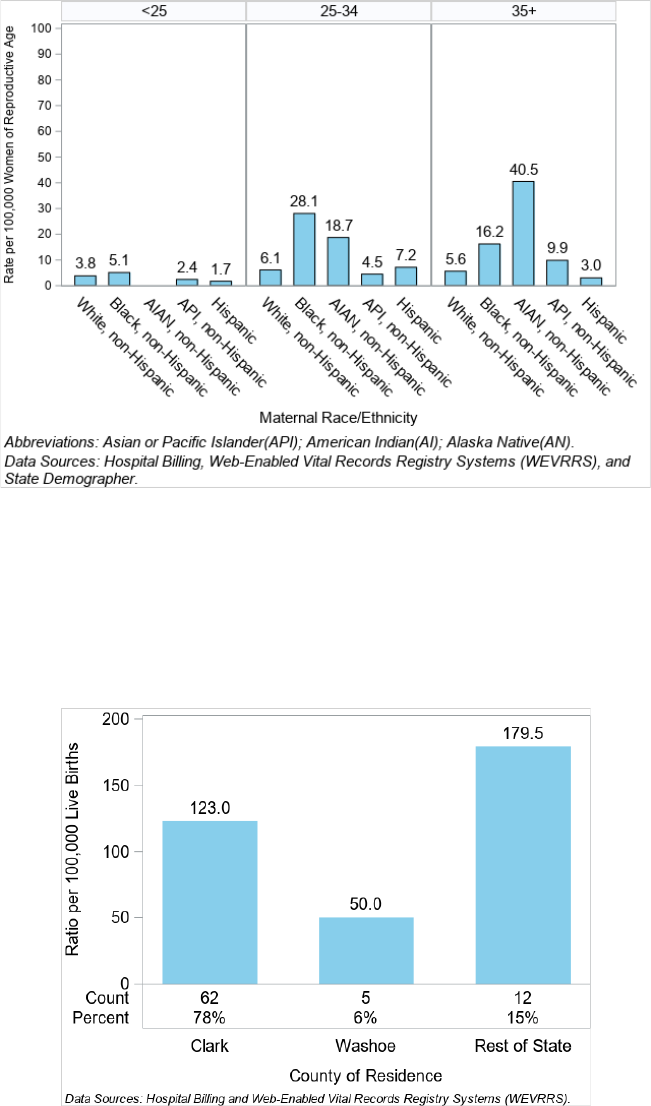
AI/AN, non-Hispanic Nevadans within the age group 35+ had the highest pregnancy-associated death rates at 40.5
per 100,000 women of reproductive age each (Figure 11).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 18
Figure 11. Pregnancy-Associated Death (PAD) Rate by Maternal Age and Race/Ethnicity, Nevada 2020-2021
Most pregnancy-associated deaths occurred in Clark County (78%) (Figure 12). However, the Rest of State category
had the highest pregnancy‐associated death ratio at 179.5 per 100,000 live births and Washoe County had the
lowest ratio at 50.0 per 100,000 live births. Counties included in the category of Rest of State were Carson City,
Churchill, Douglas, Elko, Esmeralda, Eureka, Humboldt, Lander, Lincoln, Lyon, Mineral, Nye, Pershing, Storey, and
White Pine.
Figure 12. Pregnancy-Associated Death (PAD) Ratio by County of Residence, Nevada 2020-2021
Clark County had the highest pregnancy-associated death rate at 6.4 per 100,000 women of reproductive age, if
Rest of State is excluded. (Figure 13).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 19
Figure 13. Pregnancy-Associated Death (PAD) Rate by County of Residence, Nevada 2020-2021
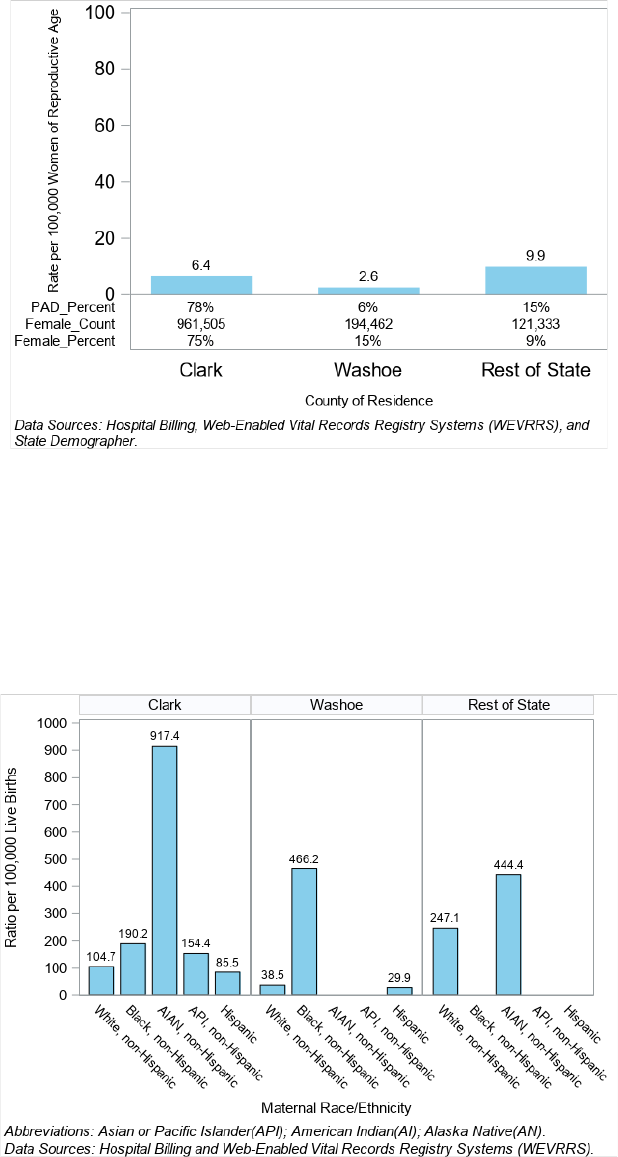
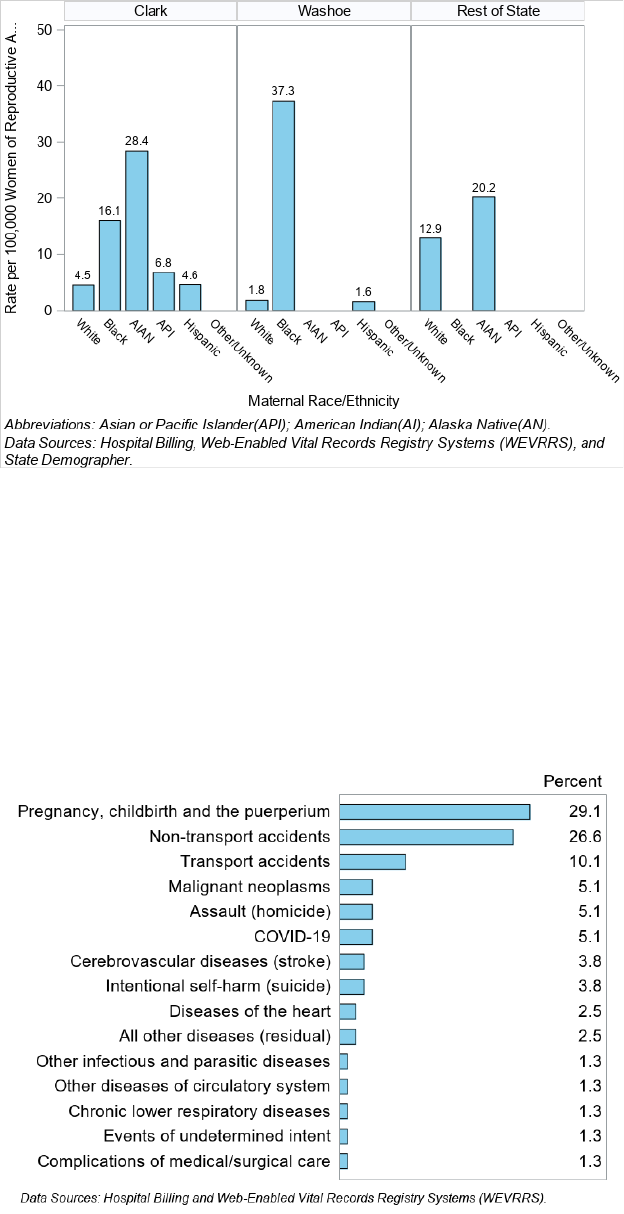
The pregnancy-associated death ratio for each race and ethnicity group within Clark County, Washoe County and
Rest of State can be seen in Figure 14. In Clark County, AI/AN, non-Hispanic Nevadans had the highest PAD ratio at
917.4 per 100,000 live births. In Washoe County, Black, non-Hispanic Nevadans had the highest PAD ratio at 466.2
per 100,000 live births. In the Rest of State, AI/AN, non-Hispanic Nevadans had the highest PAD ratio at 444.4 per
100,000 live births.
Figure 14. Pregnancy-Associated Death (PAD) Ratio by County of Residence and Maternal Race/Ethnicity, Nevada
2020-2021
In Washoe County, Black, non-Hispanic Nevadans had the highest rate of PAD at 37.3 per 100,000 women of
reproductive age (Figure 15).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 20
Figure 15. Pregnancy-Associated Death (PAD) Rate by County of Residence and Maternal Race/Ethnicity, Nevada
2020-2021
Underlying Causes of Pregnancy-Associated Deaths
During the years 2020 through 2021, the most common underlying cause of pregnancy-associated death was
Pregnancy, childbirth, and the puerperium accounting for 29.1% of all pregnancy-associated deaths. The second
most common cause of death was non-transport accidents at 26.6% of pregnancy-associated deaths; The third most
common cause of death was Transport accidents at 10.1% (Figure 16).
Figure 16. Underlying Causes of Death for Pregnancy-Associated Deaths by Percent, Nevada, 2020-2021
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 21
Table 1. Underlying Causes of Death for Pregnancy-Associated Deaths by Race/Ethnicity, Nevada, 2020-2021
Abbreviations: Asian or Pacific Islander (API); American Indian/Alaska Native (AI/AN).
Data Sources: Hospital Billing Data, Nevada Electronic Birth and Death Registry
Causes of Death
White,
non-
Hispanic
Black,
non-
Hispanic
AI/AN,
non-
Hispanic
API, non-
Hispanic
Hispanic
Other/
Unknown
Total
N
%
N
%
N
%
N
%
N
%
N
%
N
%
Pregnancy, childbirth
and the puerperium
9
31 %
5
25 %
0
0 %
2
25 %
6
33.3 %
1
100 %
23
29.1 %
Non-transport
accidents
10
34.5 %
4
20 %
1
33.3 %
1
12.5 %
5
27.8 %
0
0 %
21
26.6 %
Transport accidents
2
6.9 %
2
10 %
1
33.3 %
1
12.5 %
2
11.1 %
0
0 %
8
10.1 %
Malignant neoplasms
1
3.4 %
2
10 %
0
0 %
1
12.5 %
0
0 %
0
0 %
4
5.1 %
Assault (homicide)
0
0 %
2
10 %
0
0 %
0
0 %
2
11.1 %
0
0 %
4
5.1 %
COVID-19
1
3.4 %
1
5 %
1
33.3 %
1
12.5 %
0
0 %
0
0 %
4
5.1 %
Intentional self-harm
(suicide)
2
6.9 %
0
0 %
0
0 %
0
0 %
1
5.6 %
0
0 %
3
3.8 %
Cerebrovascular
diseases (stroke)
1
3.4 %
1
5 %
0
0 %
0
0 %
1
5.6 %
0
0 %
3
3.8 %
All other diseases
(residual)
0
0 %
1
5 %
0
0 %
0
0 %
1
5.6 %
0
0 %
2
2.5 %
Diseases of the heart
1
3.4 %
0
0 %
0
0 %
1
12.5 %
0
0 %
0
0 %
2
2.5 %
Chronic lower
respiratory diseases
1
3.4 %
0
0 %
0
0 %
0
0 %
0
0 %
0
0 %
1
1.3 %
Other infectious and
parasitic diseases
0
0 %
1
5 %
0
0 %
0
0 %
0
0 %
0
0 %
1
1.3 %
Events of
undetermined intent
1
3.4 %
0
0 %
0
0 %
0
0 %
0
0 %
0
0 %
1
1.3 %
Complications of
medical/surgical care
0
0 %
1
5 %
0
0 %
0
0 %
0
0 %
0
0 %
1
1.3 %
Other diseases of
circulatory system
0
0 %
0
0 %
0
0 %
1
12.5 %
0
0 %
0
0 %
1
1.3 %
Total
29
100 %
20
100 %
3
100 %
8
100 %
18
100 %
1
100 %
79
100 %
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 22
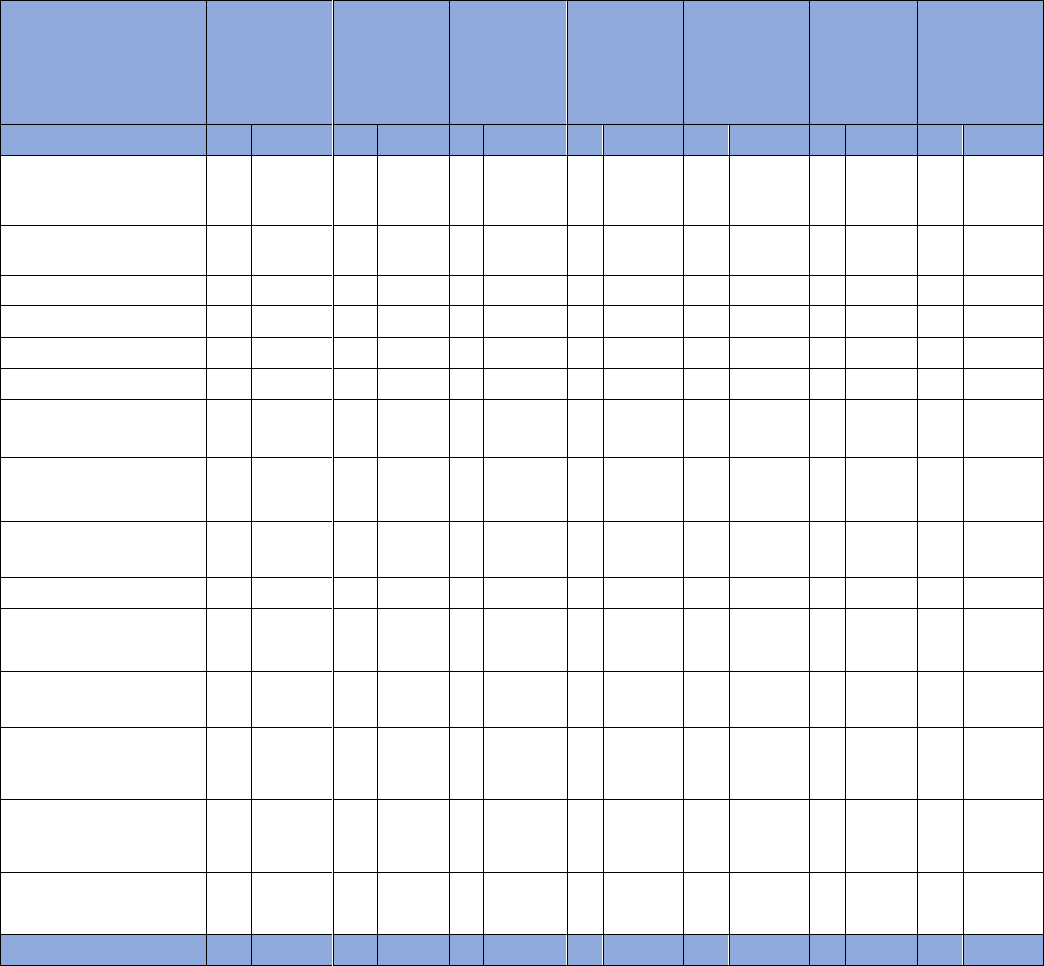
Table 2. Underlying Causes of Death for Pregnancy-Associated Deaths by County of Residence, Nevada, 2020-2021
Data Sources: Hospital Billing Data, Nevada Electronic Birth and Death Registry
Drug Overdose Deaths
Pregnancy-associated deaths can intersect with substance use-related drug overdoses. The underlying cause of
death for pregnancy-associated deaths were described above; however, additional information may be available
on the death certificate which can provide more information surrounding the circumstances of death. These
conditions are known as no underlying causes of death or multiple causes of death.
14
To identify drug overdose-related no underlying causes of death for Nevadans with confirmed pregnancy-associated
deaths, certain ICD-10 codes were looked for on the death records: X40-X44 (unintentional), X60-X64 (suicide), X85
(homicide), and Y10-Y14 (undetermined). These codes are related to the cause of death category of Injury by drug
overdose (which can refer to an overdose caused by any opioid, heroin, natural and semisynthetic opioids,
methadone, or other synthetic opioids (other than methadone)).
14
14
Centers for Disease Control and Prevention (CDC). Health, United States 2020-2021 – Cause of Death. https://www.cdc.gov/nchs/hus/sources-definitions/cause-of-death.htm
14
Centers for Disease Control and Prevention (CDC). Health, United States 2020-2021 – Cause of Death. https://www.cdc.gov/nchs/hus/sources-definitions/cause-of-death.htm
Causes of Death
Clark
Washoe
Rest of State
Total
N
%
N
%
N
%
N
%
Pregnancy, childbirth, and the
puerperium
20
32.3 %
1
20 %
2
16.7 %
23
29.1 %
Non-transport accidents
18
29 %
0
0 %
3
25 %
21
26.6 %
Transport accidents
5
8.1 %
0
0 %
3
25 %
8
10.1 %
Malignant neoplasms
3
4.8 %
1
20 %
0
0 %
4
5.1 %
Assault (homicide)
3
4.8 %
1
20 %
0
0 %
4
5.1 %
COVID-19
3
4.8 %
0
0 %
1
8.3 %
4
5.1 %
Intentional self-harm (suicide)
0
0 %
2
40 %
1
8.3 %
3
3.8 %
Cerebrovascular diseases (stroke)
3
4.8 %
0
0 %
0
0 %
3
3.8 %
All other diseases (residual)
2
3.2 %
0
0 %
0
0 %
2
2.5 %
Diseases of the heart
1
1.6 %
0
0 %
1
8.3 %
2
2.5 %
Chronic lower respiratory diseases
1
1.6 %
0
0 %
0
0 %
1
1.3 %
Other infectious and parasitic
diseases
1
1.6 %
0
0 %
0
0 %
1
1.3 %
Events of undetermined intent
0
0 %
0
0 %
1
8.3 %
1
1.3 %
Complications of medical/surgical
care
1
1.6 %
0
0 %
0
0 %
1
1.3 %
Other diseases of circulatory
system
1
1.6 %
0
0 %
0
0 %
1
1.3 %
Total
62
100 %
5
100 %
12
100 %
79
100 %
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 23
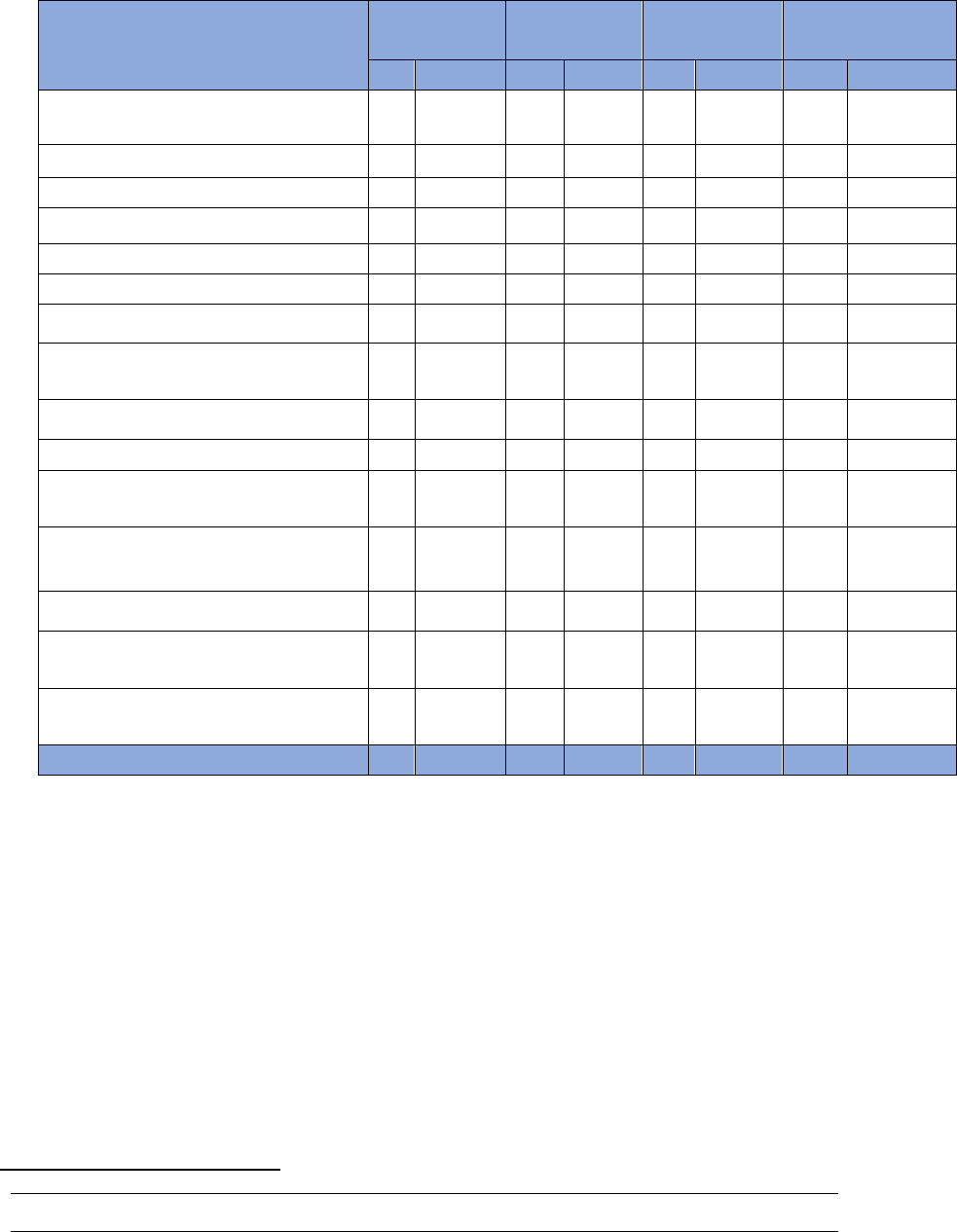
Figure 17 displays underlying causes of death for pregnancy-associated deaths that also had an ICD10 code on the
death certificate confirming Injury by drug overdose. Most drug overdoses identified in pregnancy-associated
deaths were associated with the underlying cause of death of non-transport accidents (82.6%).
Figure 17. Percent of Drug Overdoses Associated with Pregnancy-Associated Deaths by Underlying Cause of Death,
Nevada, 2020-2021
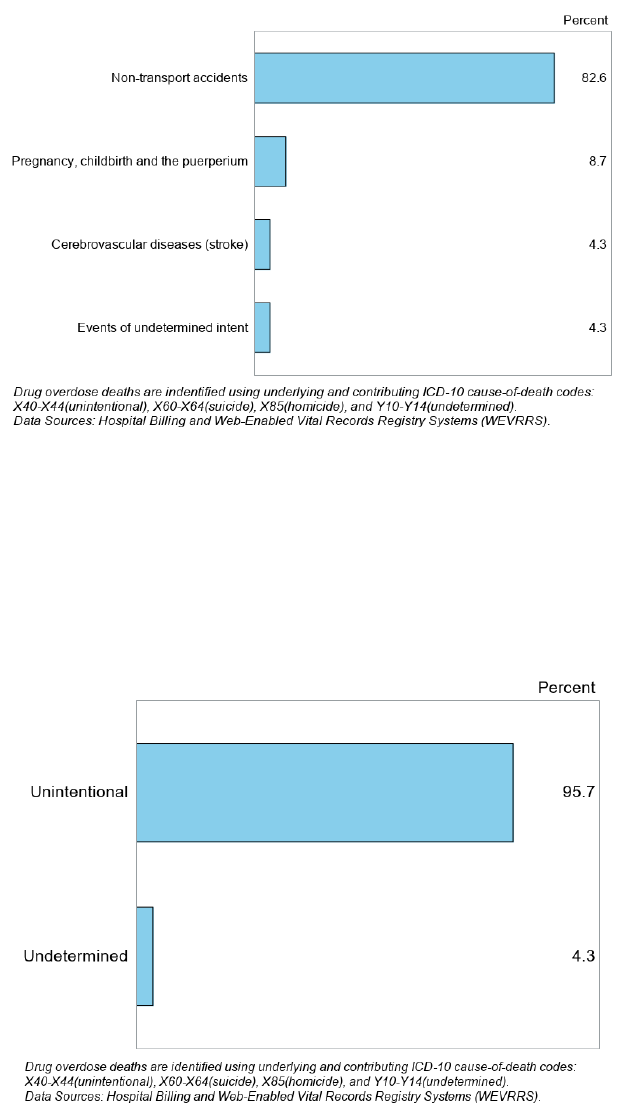
Of the drug overdoses associated with pregnancy-associated deaths, 95.7% were coded as unintentional overdoses
(Figure 18).
Figure 18. Percent of Drug Overdoses Associated with Pregnancy-Associated Deaths by Overdose Intention, Nevada,
2020-2021
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 24
Pregnancy-Related Death (PRD)
Methodology
Data Sources
Web-Enabled Vital Records Registry Systems (WEVRRS)
Statewide births, deaths, and fetal deaths are collected by the Office of Vital Records, in the Division of Public and
Behavioral Health. WEVRRS is a software utilized by physicians, registered nurses, midwives, informants or funeral
directors, and other individuals to collect and consolidate birth and death-related information.
State Demographer
The Nevada State Demographer provides the Nevada population of women of reproductive age which is used in
calculating rates.
Pregnancy Mortality Surveillance System (PMSS)
The Centers for Disease Control and Prevention (CDC) manage the PMSS which collects national data regarding
pregnancy-related deaths in the United States.
Identification of Pregnancy-Related Deaths
CDC conducts national pregnancy-related mortality surveillance to better understand the risk factors for and causes
of pregnancy-related deaths in the United States. The Pregnancy Mortality Surveillance System (PMSS) defines a
pregnancy-related death as the death of a person while pregnant or within 1 year of the end of pregnancy from any
cause related to or aggravated by the pregnancy. The Nevada Department of Health and Human Services Office of
Analytics annually provides a list of pregnancy‐associated deaths to the CDC. Medically trained epidemiologists at
the CDC review and analyze the cases provided, determine which cases meet the CDC’s definition of pregnancy‐
related mortality, and send a list of cases back to the Office of Analytics.
General Statistics
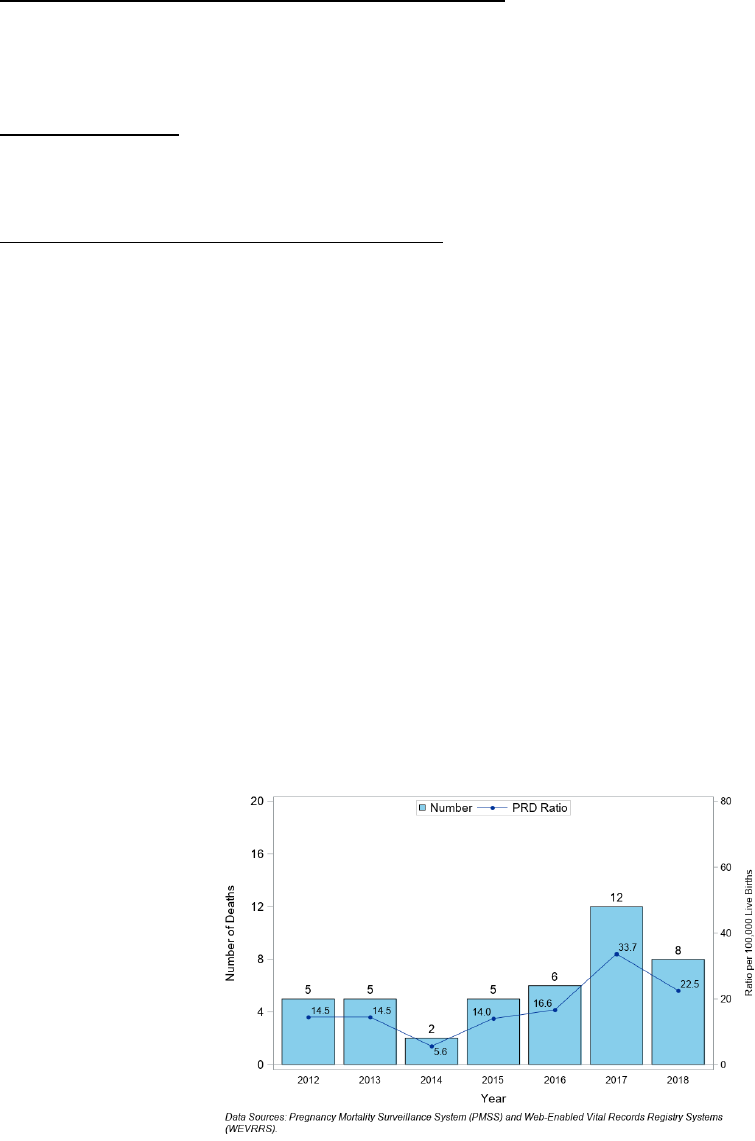
There were 43 pregnancy-related deaths for Nevada residents from 2012 to 2018 according to data from the
Pregnancy Mortality Surveillance System (total of years shown in Figure 19) -- the most recent year of data available
from PMSS is 2018. The highest ratio occurred in 2017, at 33.7 per 100,000 live births.
Figure 19. Number of Pregnancy-Related Deaths (PRD) and Death Ratio per 100,000 Live Births, Nevada, 2012 -
2018
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 25
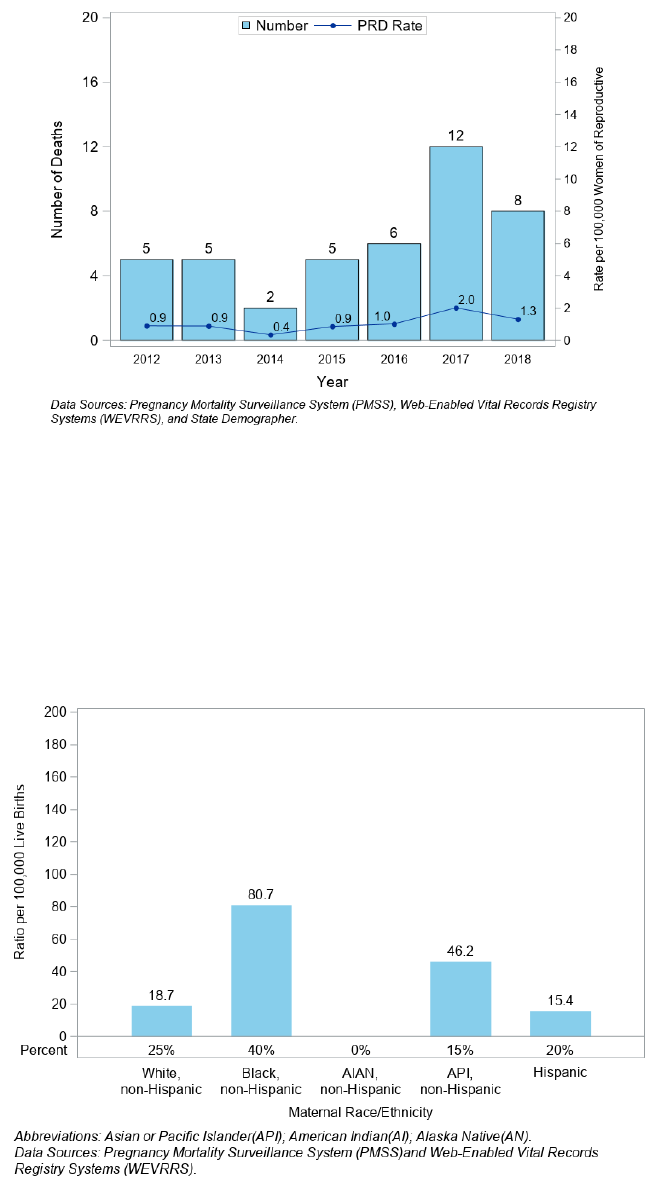
The highest pregnancy-related death rate was in 2017 at 2.0 per 100,000 women of reproductive age (Figure 20).
Figure 20. Number of Pregnancy-Related Deaths (PRD) and Death Rate per 100,000 Women of Reproductive Age,
Nevada, 2012 - 2018
Maternal Demographics
Black, non-Hispanic Nevadans had the highest pregnancy-related death ratio at 80.7 per 100,000 live births and
40% of the pregnancy-related deaths occurring between 2017 through 2018 (Figure 21). Hispanic Nevadans had the
lowest death ratio of those who died at 15.4 per 100,000 live births, accounting for 20% of all deaths. AI/AN, non-
Hispanic Nevadans had no pregnancy-related deaths in the years under review.
Figure 21. Pregnancy-Related Death (PRD) Ratio per 100,000 Live Births and Percent by Race/Ethnicity, Nevada,
2017 - 2018
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 26
Black, non-Hispanic Nevadans had the highest death rate at 7.1 per 100,000 women of reproductive age (Figure
22).
Figure 22. Pregnancy-Related Death (PRD) Rate per 100,000 Women of Reproductive Age and Percent by
Race/Ethnicity, Nevada, 2017 - 2018
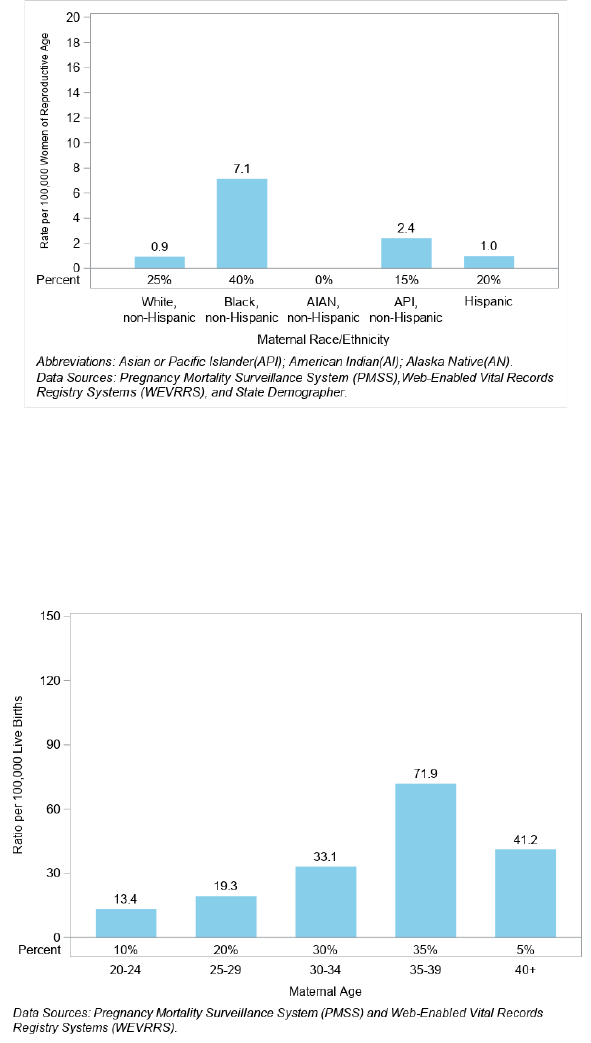
Nevadans aged 35 to 39 had the highest pregnancy-related death ratio at 71.90 per 100,000 live births, followed by
40+ age group at a ratio of 41.2 per 100,000 live births (Figure 23). Sixty-five percent of the deaths occurred among
the 30 to 39 age group in total.
Figure 23. Pregnancy-Related Death (PRD) Ratio and Percent by Maternal Age, Nevada, 2017 - 2018
For the age group 35 to 39, the highest pregnancy-related death rate was at 3.4 per 100,000 women of reproductive
age followed by the age group 30 to34 at 3.0 per 100,000 women of reproductive age (Figure 24).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 27
Figure 24. Pregnancy-Related Death (PRD) Rate and Percent by Maternal Age, Nevada, 2017 - 2018
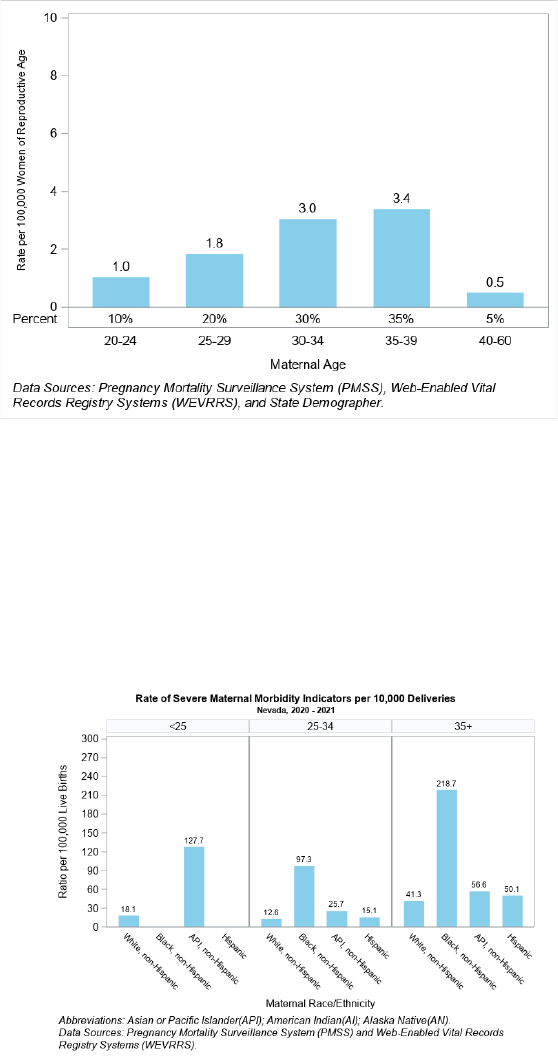
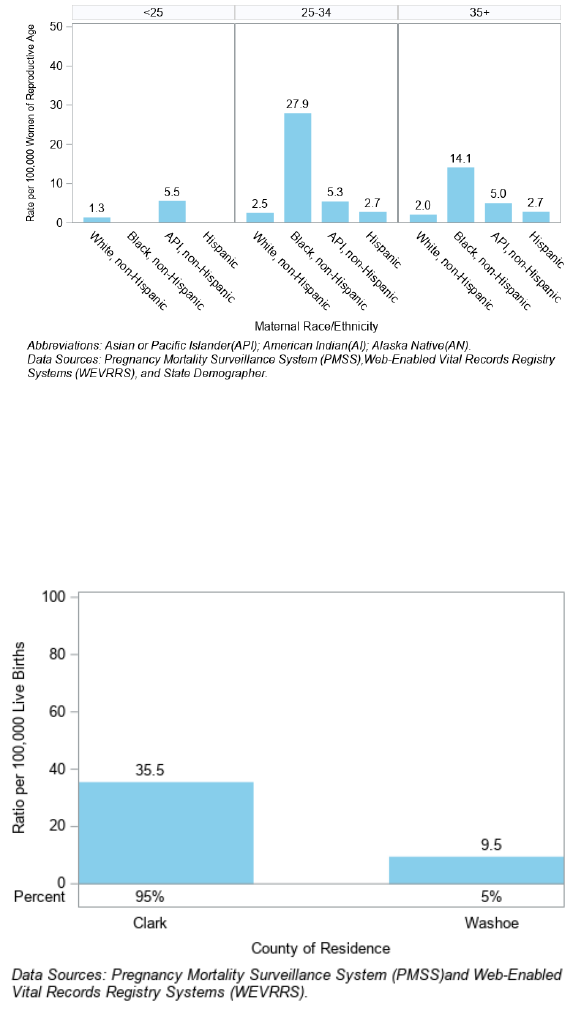
Figure 25 illustrates the pregnancy-related death ratio for each race and ethnicity within age groups of under 25,
25 to 34, and 35 and older. For ages 35 and above, Black, non-Hispanic Nevadans had the highest death ratio at
218.7 per 100,000 live births and followed by Asian/Pacific Islander (API), non-Hispanics with death ratio at 56.6 per
100,000 live births. For 25 and under, Asian/Pacific Islander (API), non-Hispanic Nevadans had the highest death
ratio at 127.7 per 100,000 live births.
Figure 25. Pregnancy-Related Death (PRD) Ratio by Maternal Age and Race/Ethnicity, Nevada, 2017 - 2018
For the age group 25 to 34, Black, non-Hispanic Nevadans had the highest death rate at 27.9 per 100,000 women
of reproductive age (Figure 26).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 28
Figure 26. Pregnancy-Related Death (PRD) Rate by Maternal Age and Race/Ethnicity, Nevada, 2017 - 2018
Clark County had the highest pregnancy-related death ratio at 35.5 per 100,000 live births, accounting for 95% of
all pregnancy-related deaths, Washoe had 5% of all pregnancy-related deaths, and Rest of State did not have any
pregnancy-related death (Figure 27).
Figure 27. Pregnancy-Related Death (PRD) Ratio by County of Residence, Nevada, 2017 - 2018
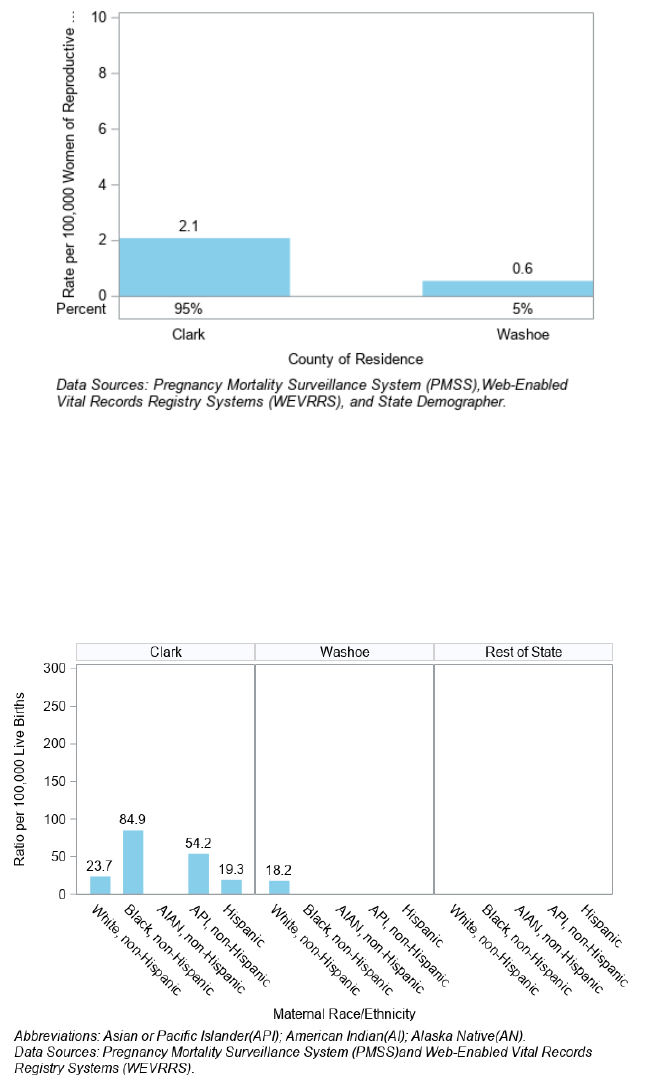
The highest pregnancy-related death rate was in Clark County at 2.1 per 100,000 women of reproductive age (Figure
28).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 29
Figure 28. Pregnancy-Related Death (PRD) Rate by County of Residence, Nevada, 2017 - 2018
Figure 29 illustrates the pregnancy-related death ratio for each race and ethnicity group within Clark County,
Washoe County and Rest of State. In Clark County, Black, non-Hispanic Nevadans had the highest ratio at 84.9 per
100,000 live births. In Washoe County, White, non-Hispanic Nevadans had the highest ratio at 18.2 per 100,000 live
births, and Rest of State did not have any pregnancy-related death. There is no ratio for AI/AN, non-Hispanic for
any of the category and Black, non-Hispanic, API, non-Hispanic and Hispanic for Washoe county.
Figure 29. Pregnancy-Related Death (PRD) Ratio by County of Residence and Race/Ethnicity, Nevada, 2017 - 2018
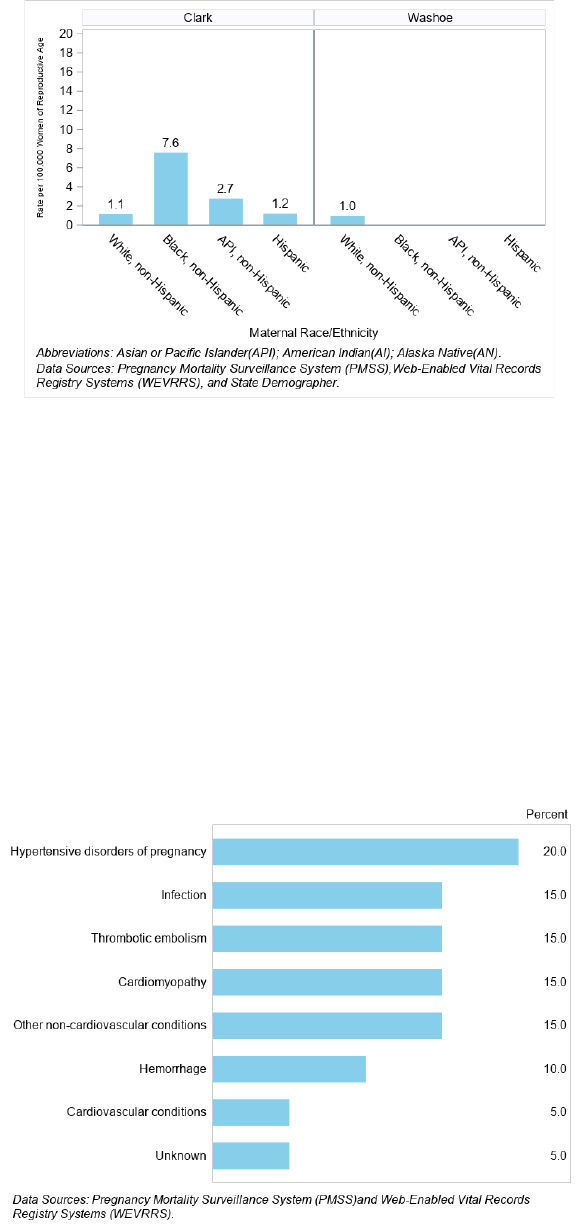
In Clark County, Black, non-Hispanic Nevadans had the highest rate at 7.6 per 100,000 women of reproductive age.
In Washoe County, White, non-Hispanic Nevadans had the highest rate at 1.0 per 100,000 women of reproductive
age and did not have any rates for other races (Figure 30).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 30
Figure 30. Pregnancy-Related Death (PRD) Rate by County of Residence and Race/Ethnicity, Nevada, 2017 - 2018
Underlying Causes of Pregnancy-Related Deaths
During 2017 and 2018, the most common causes of pregnancy-related death were Hypertensive disorders of
pregnancy, which accounted for 20% of all pregnancy-related deaths, followed by Infection, Thrombotic embolism,
Cardiomyopathy, and Other non-cardiovascular conditions each accounting for 15% respectively of all pregnancy-
related deaths.
Figure 31. Underlying Causes of Death of Pregnancy-Related Deaths, Nevada, 2017 - 2018
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 31
Table 3. Count of Pregnancy-Related Deaths by Underlying Causes of Death, Nevada, 2017 – 2018
Cause of
Death
White,
non-
Hispanic
Black, non-
Hispanic
AIAN,
non-
Hispanic
API, non-
Hispanic
Hispanic
Other/
Unknown
Total
N
%
N
%
N
%
N
%
N
%
N
%
N
%
Hypertensive
disorders of
pregnancy
0
0 %
2
25 %
0
0 %
1
33.3 %
1
25 %
0
0 %
4
20 %
Thrombotic
embolism
2
40 %
1
12.5 %
0
0 %
0
0 %
0
0 %
0
0 %
3
15 %
Cardiomyopat
hy
1
20 %
2
25 %
0
0 %
0
0 %
0
0 %
0
0 %
3
15 %
Cardiovascula
r conditions
0
0 %
0
0 %
0
0 %
0
0 %
1
25 %
0
0 %
1
5 %
Hemorrhage
0
0 %
1
12.5 %
0
0 %
1
33.3 %
0
0 %
0
0 %
2
10 %
Infection
1
20 %
0
0 %
0
0 %
1
33.3 %
1
25 %
0
0 %
3
15 %
Other non-
cardiovascula
r conditions
1
20 %
2
25 %
0
0 %
0
0 %
0
0 %
0
0 %
3
15 %
Unknown
0
0 %
0
0 %
0
0 %
0
0 %
1
25 %
0
0 %
1
5 %
Total
5
100 %
8
100 %
0
0 %
3
100 %
4
100 %
0
0 %
20
100 %
AI/AN stands for American Indian Alaska Native, and API is Asian Pacific Islander.
Data Sources: Pregnancy Mortality Surveillance System (PMSS), Nevada Electronic Birth Registry.
Table 4. Count of Pregnancy-Related Deaths by Underlying Causes of Death by County, Nevada, 2017 - 2018
Cause of Death
Clark
Washoe
Rest of
State
Total
N
%
N
%
N
%
N
%
Hypertensive disorders of pregnancy
4
21.1 %
4
20 %
Thrombotic embolism
3
15.8 %
3
15 %
Cardiomyopathy
3
15.8 %
3
15 %
Cardiovascular conditions
1
5.3 %
1
5%
Hemorrhage
2
10.5 %
2
10 %
Infection
2
10.5 %
1
100%
3
15 %
Other non-cardiovascular conditions
3
15.8 %
3
15 %
Unknown
1
5.3 %
1
5 %
Total
19
100%
1
5 %
20
100 %
Data Sources: Pregnancy Mortality Surveillance System (PMSS), Nevada Electronic Birth Registry.
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 32
Maternal Deaths
Methodology
Data Sources
Data sources used to identify maternal deaths are the same as those used to identify pregnancy-related deaths.
Identification of Maternal Deaths
Methodology to identify maternal deaths is based upon that used to identify pregnancy-related deaths but is
restricted to individuals who died while pregnant or within 42 days of the termination of pregnancy, regardless of
the duration and site of pregnancy, from any cause related to or aggravated by the pregnancy or its management,
but not from accidental or incidental causes regardless of the duration and site of pregnancy, from any cause
related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.
General Statistics
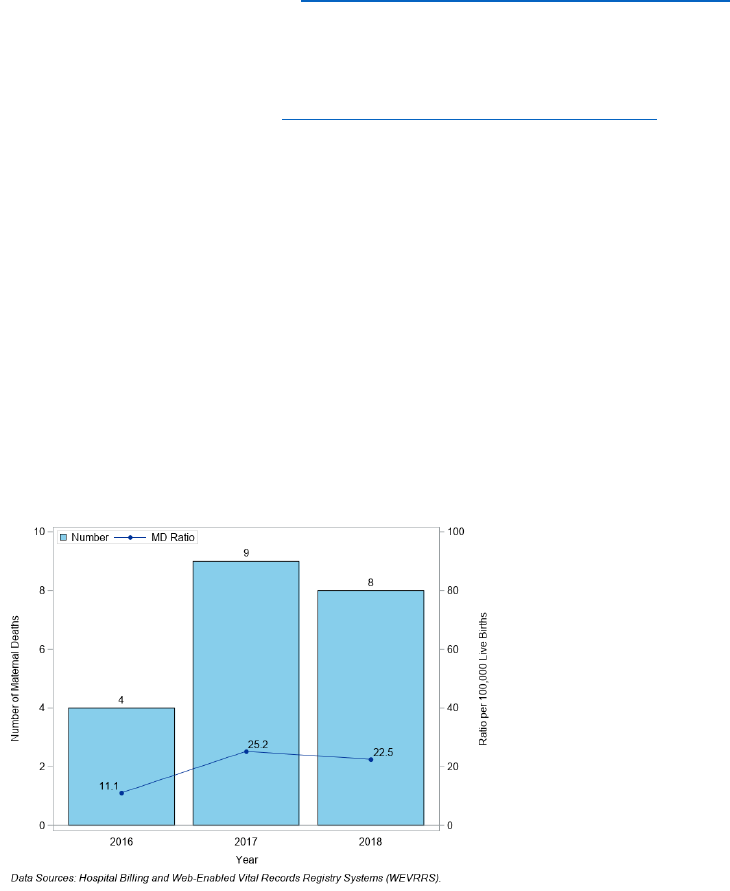
There were 21 maternal deaths in Nevada from 2016 to 2018 (sum of counts by year in Figure 32).
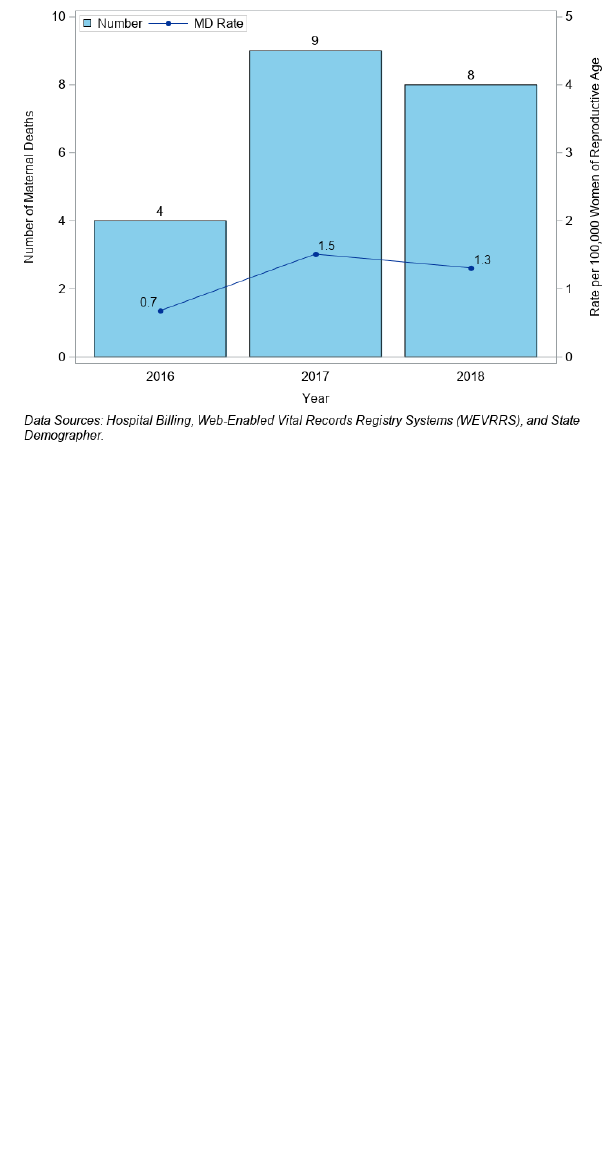
The highest ratios were in 2017 at 25.2 per 100,000 live births (Figure 32) and a rate of 1.5 per 100,000 women of
reproductive age (Figure 33).
Figure 32. Number of Maternal Deaths (MD) and Death Ratio per 100,000 Live Births, Nevada, 2016-2018
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 33
Figure 33. Number of Maternal Deaths (MD) and Death Rate per 100,000 Women of Reproductive, Nevada, 2016-
2018
Maternal Demographics
A total of 21 Nevadans had a maternal death during 2016 to 2018. By race and ethnicity, the Nevadans who died
were 7 White, non‐Hispanic, 6 Black, non‐Hispanic, 2 Asian/Pacific Islander and 6 Hispanic. There are 9 Nevadans
for the age group 24 to 34 and 12 for age group 35 to 45.
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 34
Severe Maternal Morbidity (SMM) Data
Definition
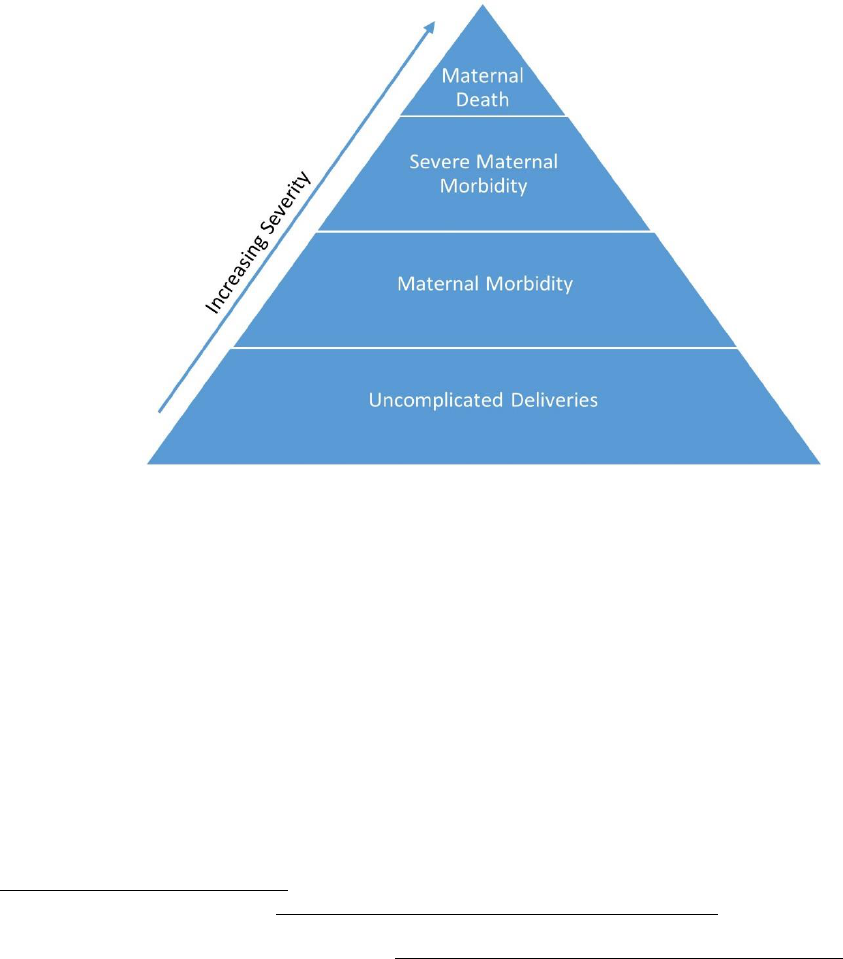
As noted in the Background section of this report, maternal morbidity is a continuum from mild adverse
effects to life‐threatening events or death.2 above
2
Severe Maternal Morbidity (SMM) refers to conditions
and diagnoses which indicate potentially life-threatening maternal complications. SMM includes
unexpected outcomes of labor and delivery resulting in significant short‐ or long‐term consequences to
health.
3
Figure 33 below illustrates the maternal morbidity continuum.
Figure 34. Maternal Morbidity Continuum
National Severe Maternal Mortality Statistics
The Centers for Disease Control and Prevention (CDC) reports that SMM has been steadily increasing in
recent years and affected more than 50,000 pregnant people in the United States in 2014 (according to
most recent publicly available data).
11
The overall rate of SMM per 10,000 deliveries increased almost 200%
over the years, from 49.5 in 1993 to 144.0 in 2014.
11
Blood transfusions play a primary role in the national increase of SMM.
11
A blood transfusion refers to the
procedure in which pregnant people are given donated blood around their delivery hospitalization. The
rate of blood transfusions per 10,000 deliveries increased from 24.5 in 1993 to 122.3 in 2014
11
which likely
affects the increase in SMM among those receiving blood transfusions. Excluding blood transfusions, the rate of SMM per
10,000 deliveries still increased by 20% in the same timeframe (from 28.6 per 10,000 deliveries in 1993 to 35.0
2
Severe Maternal Morbidity, New York City, 2008‐2012. https://www1.nyc.gov/assets/doh/downloads/pdf/data/maternal‐morbidity‐report‐08‐12.pdf
3
American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine, Kilpatrick SK, Ecker JL. Severe maternal morbidity: screening and review. Am J Obstet
Gynecol. 2016;215(3): B17–B22.
11
Centers for Disease Control and Prevention (CDC). Severe Maternal Morbidity. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 35
per 10,000 deliveries in 2014).
11
Methodology
Data Sources
Nevada Electronic Birth Registry Data
Nevada Department of Health and Human Services, Office of Vital Records used Web‐enabled Vital
Records Registry System (WEVRRS) to collect information on all live births in Nevada and issue birth
certificates. The birth certificate contains demographic information, such as the mother’s age, race,
education, and pregnancy information, such as parity and prenatal care.
Hospital Inpatient Billing (HIB) Data
The Hospital Inpatient Billing data provides health billing data for patients discharged from Nevada’s non‐
federal hospitals. NRS 449.485 mandates all hospitals in Nevada report discharge information as
prescribed by the director of the Department of Health and Human Services. The data are collected using
a standard universal billing form. The data are for patients admitted for at least 24 hours as an inpatient
but do not include patients discharged from the emergency room. The data consists of demographics such
as age, gender, race/ethnicity and uses International Classification of Diseases‐10‐Clinical 5 Modification
(ICD‐10‐CM) diagnoses (up to 33 diagnoses respectively). In addition, the data includes billed hospital
charges, procedure codes, length of hospital stay, discharge status, and external cause of injury codes.
The billing data information is for billed charges and not the actual payment received by the hospital.
Identification of Severe Maternal Morbidity
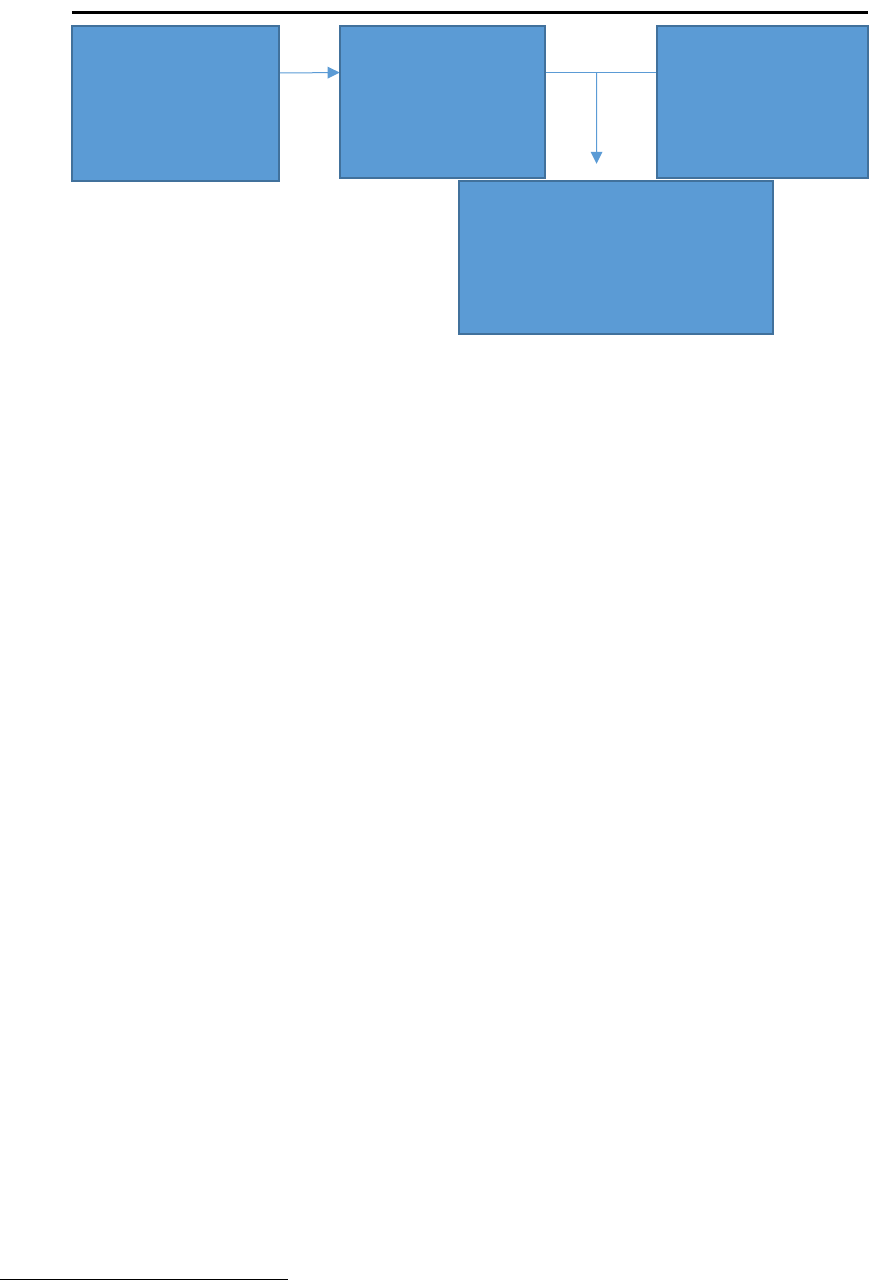
Nevada birth certificates were matched with the mother’s delivery hospitalization record from Hospital
Inpatient Billing (HIB) data. Multiple births (e.g., twins, triplets) were counted as one delivery (only one
birth certificate was matched per hospital discharge record, even with multiple births). The total number
of live births to Nevada residents was 66,043 from January 2020 to December 2021. The total number of
deliveries was 63,528, comprising all records from singleton births and one record per multiple births.
Approximately 95.7% of all deliveries were matched with a hospital discharge record. All analyses are
based on matched data (N=60,813). Birth certificates and hospital discharge records were matched with
the mother’s social security number, name, birth date, medical record number, and the facility of the
delivery hospitalization. Non‐matched birth certificates may be due to home births, missing social security
numbers, misspelled names, etc.
11
Centers for Disease Control and Prevention (CDC). Severe Maternal Morbidity. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 36
Figure 35. Data Matching Process for Birth Certificates and HIB Records, Nevada, 2020-2021
SMM events were identified during delivery hospitalizations using an algorithm developed by researchers
at the CDC.
12
The algorithm used ICD‐9/10‐CM codes to identify 25 indicators of SMM that represent either
serious complications of pregnancy or delivery, such as disseminated intravascular coagulation or
eclampsia, or procedures used to manage serious conditions, such as blood transfusion or hysterectomy.
The Alliance for Innovation on Maternal Health (AIM) methods were used to identify pregnancy deliveries,
and ICD‐9 was converted to ICD‐10 to identify SMM indicators. Four out of 25 ICD‐9 indicators did not have
corresponding ICD‐10 codes. Of the 21 indicators remaining, 16 were identified using ICD‐10 diagnosis
codes, and five were identified using ICD‐10 procedure codes. A complete list of conditions and ICD‐10
codes is listed in Appendix A.
To ensure that only the most severe cases of these 21 indicators during delivery hospitalizations were
captured, these indicators were classified as SMM only if they additionally met one of the following criteria:
•
The mother’s length of stay was equal to or greater than the 90
th
percentile by delivery method.
•
The mother was transferred before or after delivery to a different facility.
•
The mother died during delivery hospitalization.
•
At least one of the five procedure indicators was present.
Analysis
All SMM rates were calculated per 10,000 live deliveries that successfully matched with a HIB record. Chi-
square tests and bivariate logistic regression were used to test the significance of the association between
maternal characteristics and SMM. The analyses in this report include blood transfusion in SMM calculation
unless otherwise noted. P‐values less than 0.05 were deemed statistically significant.
Records with missing data on a variable of interest were not represented in the graph of SMM but are
represented in the tables.
All analyses were conducted using SAS 9.4.
12
Callaghan WM, Creanga AA, Kuklina EV. Severe Maternal Morbidity Among Delivery and Postpartum Hospitalizations in the United States. Obstetrics and Gynecology 2012; 120:1029‐36.
All live birth
certificates Nevada
residents, 2020 -
2021
N = 66,043
All deliveries of
Nevada residents,
2020-2021
N = 63,528
HIB hospital
discharge records,
Nevada,
2020-2021
Matched birth-HIB records,
2020-2021
N = 60,813
95.7% of all deliveries
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 37
General Statistics
Between January 2020 to December 2021, there were 1,168 identified SMM cases in Nevada.
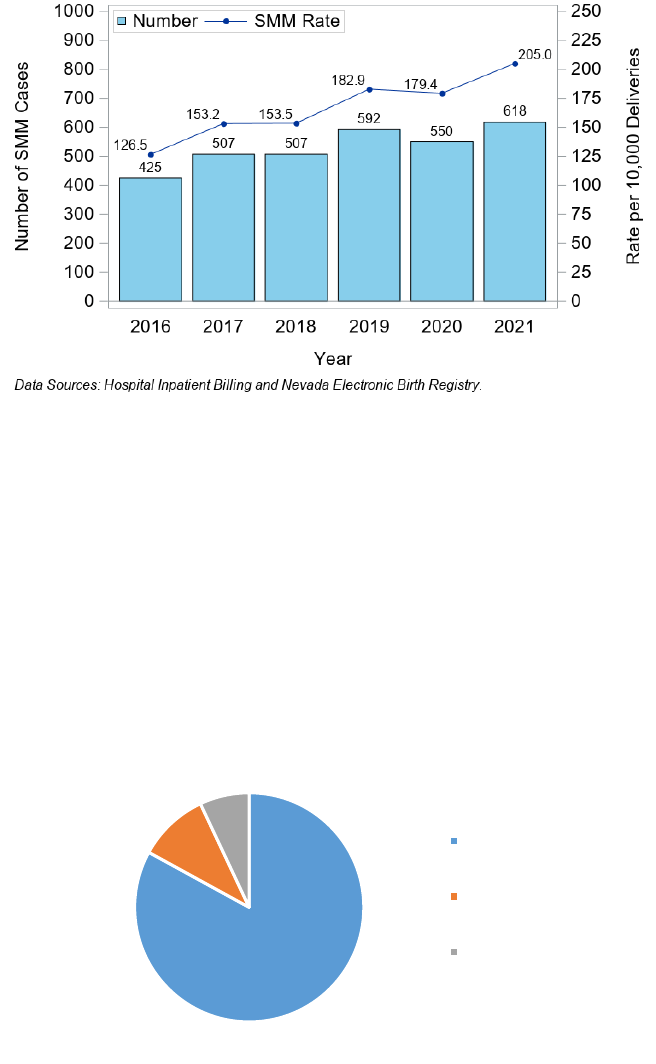
The SMM rate in Nevada increased during 2016 to 2021 from 126.5 to 205.0, with the highest rate in 2021,
at 205.6 per 10,000 deliveries with a total of 618 cases in that year (Figure 36).
Figure 36. Severe Maternal Morbidity (SMM) Rate per 10,000 Deliveries and Number of Cases, Nevada, 2016 - 2021
Indicators Associated with SMM
There are 21 procedure-based or diagnosis-based indicators associated with SMM (list available in Table
5). See Appendix A for a complete list including the ICD or procedure codes used to identify these SMM
indicators.
Most deliveries with SMM during 2020 to 2021 were associated with one indicator (83%), although 10% of
deliveries during this time were associated with two indicators, and 7% had three or more indicators
present (Figure 37).
Figure 37. Distribution of Severe Maternal Morbidity (SMM) Indicators, Nevada, 2020 - 2021
83%
10%
7%
One Indicator
Two Indicators
Three or More
Indicators
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 38
Table 5 below displays the rates of SMM per 10,000 deliveries during 2020 to 2021 by diagnosis-based and
procedure-based indicators.
The top five diagnosis-based indicators of SMM during these years were Adult respiratory distress syndrome
(28.1 per 10,000 deliveries), Sepsis (13.5 per 10,000 deliveries), Disseminated intravascular coagulation
(13.2 per 10,000 deliveries), Acute renal failure (12.5 per 10,000 deliveries), and Shock (9.7 per 10,000
deliveries). Around 52% of adult respiratory distress syndrome cases were confirmed COVID-19 cases in
these two years.
12
Table 5. Rate of Severe Maternal Morbidity (SMM) by Diagnosis-Based and Procedure-Based Indicators per 10,000
Deliveries, Nevada, 2020 – 2021
SMM Indicator
Rate per 10,000 deliveries
Diagnosis-Based Indicators
Adult respiratory distress syndrome*
28.1
Sepsis
13.5
Disseminated intravascular coagulation
13.2
Acute renal failure
12.5
Shock
9.7
Eclampsia
8.9
Pulmonary edema
6.4
Thrombotic embolism
3.3
Puerperal cerebrovascular disorders
2.1
Acute myocardial infarction
1.6
Cardiac arrest/ventricular fibrillation
1.5
Sickle cell anemia with crisis
1.0
Aneurysm
0.5
Severe anesthesia complications
0.2
Procedure-Based Indicators
Blood transfusion
141.9
Hysterectomy
19.9
Ventilation
10.4
Conversion of cardiac rhythm
1.2
Temporary tracheostomy
0.7
SMM with Blood Transfusion Rate
192.1
* Around 52% of adult respiratory distress syndrome SMM cases were confirmed COVID-19
cases in these two years.13
The top three leading procedure-based indicators of SMM were Blood transfusion (141.9 per 10,000 deliveries),
Hysterectomy (19.9 per 10,000 deliveries), and Ventilation (10.4 per 10,000 deliveries).
Blood transfusion is often associated with SMM as shown in national data previously mentioned. The 1,168 SMM
cases identified in Nevada during January 2020 through December 2021 included all cases associated with blood
transfusions. When excluding cases associated with blood transfusions, the SMM case count dropped to 414 and
the rate decreased from 192.1 to 68.1 per 10,000 deliveries (Figure 38).

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 39
Figure 38. Severe Maternal Morbidity (SMM) Rate per 10,000 Deliveries and Number of Cases by Blood Transfusion
Indicator, Nevada, 2020 - 2021
Maternal Demographics
When comparing the race and ethnicity of pregnant Nevadans among the 1,168 SMM cases identified during 2020
to 2021 and excluding the Unknown category, Black, non-Hispanic Nevadans had the highest rate of SMM at
282.2 per 10,000 deliveries (Figure 39). The second highest group was AI/AN, non-Hispanic Nevadans with an
SMM rate of 277.8 per 10,000 deliveries. Black and AI/AN, non-Hispanic pregnant Nevadans only accounted for
21% and 1% of all SMM cases. Hispanic Nevadans accounted for the highest proportion of SMM cases (36%)
followed by White, non-Hispanic (28%). Hispanic and White, non-Hispanic had the lowest rates of SMM (194.8
and 159.5 per 10,000 deliveries).
Figure 39. Severe Maternal Morbidity (SMM) Rate and Percent by Maternal Race/Ethnicity, Nevada, 2020 - 2021
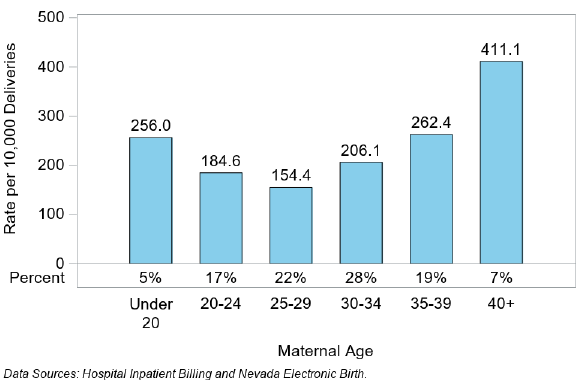
When stratifying SMM cases by age groups, although the 40 years and older age group only accounted for 7% of all
SMM cases, they had the highest SMM rate of 411.1 per 10,000 deliveries (Figure 40). The 25-29 age group
accounted for approximately 22% of SMM cases and had the lowest rate of SMM (154.4 per 10,000 deliveries).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 40
Figure 40. Severe Maternal Morbidity (SMM) Rate and Percent by Maternal Age, Nevada, 2020 - 2021
Table 6 shows the comparisons of maternal demographic characteristics among SMM cases. When
considering the SMM rate including blood transfusions, the SMM is significantly associated with maternal
age (p < 0.0001), maternal race and ethnicity (p < 0.0001), education (p = 0.0030), and health insurance
status (p = 0.0018).
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 41
Table 6. Severe Maternal Morbidity by Maternal Demographics, Nevada, 2020 – 2021
Maternal
Demographics
SMM
Cases
Rate per
10,000
Deliveries
Count of
All
Deliveries
Percent
of All
Deliveries
Percent
of SMM
Cases
Chi-
Square
P-value
Maternal Age (Years)
<=19
58
213.3
2,719
4.5 %
5 %
<0.0001
20-24
198
169.1
11,707
19.3 %
17 %
25-29
289
160.8
17,978
29.6 %
24.7 %
30-34
321
188.2
17,052
28 %
27.5 %
35-39
224
245.5
9,126
15 %
19.2 %
>=40
78
350.2
2,227
3.7 %
6.7 %
Race/ Ethnicity
White
330
152
21,707
35.7 %
28.3 %
<0.0001
Black
262
279.9
9,359
15.4 %
22.4 %
Native American
12
244.4
491
0.8 %
1 %
Asian
133
230.3
5,774
9.5 %
11.4 %
Hispanic
419
181.3
23,105
38 %
35.9 %
Other
0
0
118
0.2 %
0 %
Unknown
12
470.6
255
0.4 %
1 %
Education
Less than High
School
177
215.1
8,228
13.5 %
15.2 %
0.003
High School
Graduate
411
202.2
20,325
33.4 %
35.2 %
Some College
292
171.9
16,990
27.9 %
25 %
College Graduate or
Higher
212
159
13,331
21.9 %
18.2 %
Unknown
76
392.8
1935
3.2 %
6.5 %
Health Insurance Status*
Medicaid
568
209.6
27,105
44.6 %
48.6 %
0.0018
Other Government
30
276
1,087
1.8 %
2.6 %
Private
522
171.2
30,499
50.2 %
44.7 %
Self-pay
30
198.3
1,513
2.5 %
2.6 %
Other
13
270.8
480
0.8
1.1
Unknown
5
400
125
0.2
0.4
* Health Insurance status indicates the primary payer for the delivery as recorded on hospital
discharge form.
Table 7 shows that the SMM rate including blood transfusions is significantly associated with prenatal care
initiation (p=< 0.0001), adequacy of prenatal care (p = <0.0001), parity (p = 0.0105), method of delivery (p
= <0.0001), plurality (p = <0.0001), and chronic disease status (p = <0.0001).

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 42
Table 7. Severe Maternal Morbidity by Maternal Prenatal and Delivery-Related Characteristics, Nevada, 2020 – 2021
Maternal Prenatal
and Delivery-
Related
Characteristics
SMM
Cases
Rate per
10,000
Deliveries
Count of
All
Deliveries
Percent
of All
Deliveries
Percent
of SMM
Cases
Chi-
Square
P-value
Prenatal Care Initiation
No Care
60
424.9
1,412
2.3 %
5.1 %
<0.0001
First Trimester
775
168.4
46,012
75.7 %
66.4 %
Second Trimester
164
195.5
8,387
13.8 %
14 %
Third Trimester
48
285
1,684
2.8 %
4.1 %
Had Care but
Unknown Start Date
9
205.9
437
0.7 %
0.8 %
Unknown
112
389.3
2,877
4.7 %
9.6 %
Adequacy of Prenatal Care
Data
Missing/Unknown
185
385
4,805
7.9 %
15.8 %
<0.0001
Inadequate
135
229.4
5,884
9.7 %
11.6 %
Intermediate
82
153
5,361
8.8 %
7 %
Adequate
328
136.7
23,998
39.5 %
28.1 %
Adequate Plus
438
211
20,761
34.1 %
37.5 %
Parity
0 Previous Live
Births
465
198.8
23,393
38.5 %
39.8 %
<0.0001
1 Previous Live
Births
253
143.9
17,579
28.9 %
21.7 %
2+ Previous Live
Births
447
225.9
19,787
32.5 %
38.3 %
Unknown
3
600
50
0.1 %
0.3 %
Method of Delivery*
Repeat Cesarean
317
317.3
9,989
16.4 %
27.1 %
<0.0001
Primary Cesarean
456
437.7
10,418
17.1 %
39 %
Vaginal
395
97.8
40,402
66.4 %
33.8 %
Plurality
Singleton Birth
1096
183.2
59,820
98.4 %
93.8 %
<0.0001
Multiple Birth
72
728
989
1.6 %
6.2 %
Pre-Pregnancy BMI~
Underweight (<18.5)
36
175.4
2,052
3.4 %
3.1 %
0.2207
Normal Weight
(18.5- 24.9)
420
176.1
23,851
39.2 %
36 %
Overweight (25.0 -
29.9)
274
171.2
16,008
26.3 %
23.5 %
Class I (30.0 - 34.9)
198
206.4
9,591
15.8 %
17 %
Class II (35.0 - 39.9)
95
207.7
4,573
7.5 %
8.1 %
Class III (>=40)
63
201.5
3,126
5.1 %
5.4 %
Unknown
82
510
1,608
2.6 %
7 %
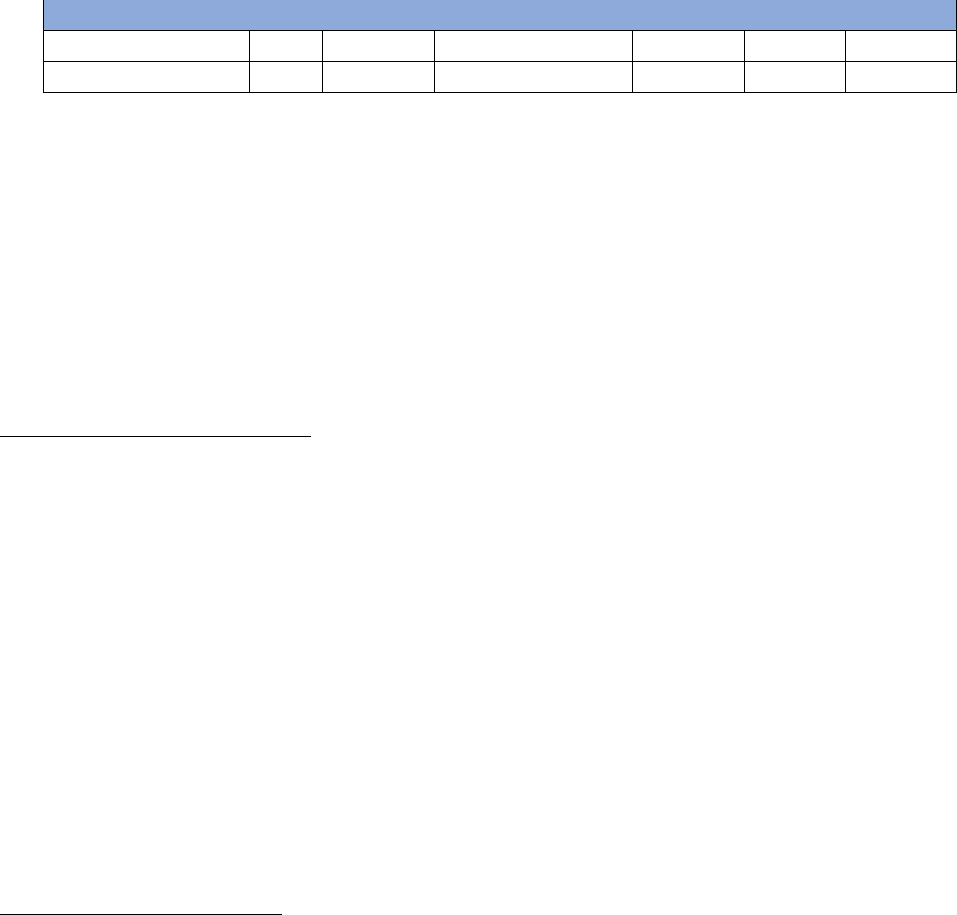
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 43
Chronic Disease^
No Chronic Disease
77
404.4
1,904
3.1 %
6.6 %
<0.0001
Any Chronic Disease
1091
185.2
58,905
96.9 %
93.4 %
*Method of delivery was identified from hospital discharge data using ICD-10 codes. Four
indicators were not carried over to ICD-10-CM codes system from ICD -9-CM
~ Pre-pregnancy BMI was calculated using the formula (weight(lb.)/height(in)^2) *703 with
mother's weight and height as recorded on birth certificate.
^ Any chronic disease includes deliveries to pregnant people with chronic hypertension, pre-
existing diabetes or chronic heart disease as recorded on birth certificate.
Data Summary
Maternal Mortality
Pregnancy-Associated Death (PAD)
The pregnancy-associated death ratios in the years 2020 and 2021 have increased from the ratios in 2016-
2019 (from a low of 60.0 per 100,000 live births in 2019 to a high of 119.1 per 100,000 births in 2020).
Pregnancy-associated deaths rate have increased from 3.4 per 100,000 live births in 2019 to 6.3 per
100,000 live births in 2020 and then a slight decrease at 6.1 in 2021.
In the years 2020 to 2021, AI/AN, non-Hispanic Nevadans had the highest pregnancy-associated death ratio
at 501.7 per 100,000 live births followed by Black, non-Hispanic Nevadans at 199.4 per 100,000 live births.
Nevadans with a maternal age of 35 and older accounted for 37% of pregnancy-associated deaths, and the
40 to 60 age group had the highest pregnancy‐associated death ratio at 487.0 per 100,000 live births.
The most common underlying cause of death was Pregnancy, childbirth, and the puerperium, accounting
for 29.1% of all pregnancy-associated deaths. The second most common cause of death was non-transport
accidents at 26.6% of pregnancy-associated deaths.
Pregnancy-Related Death (PRD)
The pregnancy-related death data is available through 2018; the highest PRD death ratio occurred in 2017,
at 33.7 per 100,000 live births increasing from previous years. The highest pregnancy-related death rate
was also in 2017 at 2.0 per 100,000 women of reproductive age.
During 2017 to 2018, Black, non-Hispanic Nevadans had the highest pregnancy-related death ratio at 80.7 per 100,
000 live births and 40% of the pregnancy-related deaths occurring in this time. Black, non-Hispanic Nevadans had
the highest death rate at 7.1 per 100,000 women of reproductive age.
Nevadans aged 35-39 had the highest PRD ratio at 71.90 per 100,000 live births, followed by 40+ age group
at a ratio of 41.2 per 100,000 live births
During 2017 and 2018, the most common underlying causes of pregnancy-related death were Hypertensive
disorders of pregnancy, which accounted for 20% of all pregnancy-related deaths, followed by Infection, Thrombotic
embolism, Cardiomyopathy, and Other non-cardiovascular conditions each accounting for 15% respectively of all
pregnancy-related deaths.

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 44
Maternal Deaths
There were 21 maternal deaths in Nevada from 2016 to 2018.
The highest ratios were in 2017 at 25.2 per 100,000 live births and a rate of 1.5 per 100,000 women of
reproductive age.
By race and ethnicity, the Nevadans who died were 7 White, non‐Hispanic, 6 Black, non‐Hispanic, 2
Asian/Pacific Islander and 6 Hispanic. There are 9 Nevadans for the age group 24 to 34 and 12 for age group
35 to 45.
Severe Maternal Morbidity
Nevada’s severe maternal morbidity (SMM) rate has increased from 2016 to 2021 with this highest rate in 2021 at
205.0 per 10,000 deliveries.
Most deliveries with SMM in 2020 to 2021 were associated with one indicator (83%). The top three leading
diagnosis-based indicators for SMM were Adult respiratory distress syndrome (52% of these were confirmed
COVID cases), Sepsis, and Disseminated intravascular coagulation. The leading procedure-based indicator was
Blood transfusion.
When comparing maternal demographic characteristics, maternal age, race/ethnicity, health insurance status,
adequacy of prenatal care, parity, method of delivery, plurality, and chronic disease are all risk factors for severe
maternal morbidity.
Black, non-Hispanic Nevadans accounted for 21% of SMM cases but had the highest SMM rate followed by AI/AN,
non-Hispanic Nevadans who accounted for 1% of SMM cases (282.2 and 277.8 per 10,000 deliveries, respectively).
Nevadans aged 40 years and older had the highest rate of SMM (411.1 per 10,000 deliveries) but accounted for
only 7% of cases. The 25 to 29 age group had the lowest rate of SMM (154.4 per 10,000 deliveries) and accounted
for 22% of cases.
Maternal Mortality Reviewed by the MMRC
Nevada MMRC members volunteer significant amounts of their time and invaluable expertise as subject matter
experts. Their dedication and hard work are deeply appreciated in service to the State and to ending preventable
maternal mortality. Members convened six times in 2021 and 2022. Case abstraction takes roughly 20 hours per
death review but often exceed this amount. Requested records can take weeks to be fulfilled and a single case
may generate numerous records requests to capture all information needed to ensure a complete abstraction.
The Committee reviewed 20 maternal mortality cases from calendar year 2019. Demographic and case
characteristics data are suppressed to ensure the identity of those whose deaths were reviewed are protected
given the small sample size. Future biennial reports will not be suppressed in relation to case characteristic data
as there will be more cases reviewed and MMRC case review trend data to consider given the MMRC is now fully
staffed, and reviews are happening at a steady pace. This will include new information available to MMRCs
including social determinants of health and access to care for each case reviewed.

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 45
Case abstraction has been supplemented with qualitative informant interviews as of November 2022 to better
address elements related to social determinants of health, racism, and discrimination. Time-limited Centers for
Disease Control and Prevention (CDC) Health Disparities funding (Federal Grant Number NH75OT000092) from
the DPBH Chronic Disease Prevention and Health Promotion Section is supporting the informant interviewers.
MMRC staff deeply appreciate the participation of family members and loved ones in sharing crucial information
in relation to their incalculable loss of a loved one to maternal mortality.
MMRC Recommendations
The Committee identified recommendations to improve care in Nevada and to improve the work of the
Committee and identified perceived level of impact if implemented (giant through small) and level (system,
facility, etc.) at which the recommendation would be implemented, per CDC best practices. Implementation of
these recommendations would decrease preventable MM and SMM in Nevada through a range of interventions
spanning medical best practices, systems level changes, social services and referral pathways, disparity and bias
reduction to increase birth equity, and through policy recommendations. Recommendations were generated by
MMRC members in relation to a specific MM case review based of the facts available. Several general
recommendations of the MMRC follow, below.
Giant Impact Recommendations
1. Availability of mental health services: state agencies funding housing services should use housing-first
treatment plans and pregnant women should be moved to the front of the list by July 1, 2024. (Level:
Facility)
2. State of Nevada agencies and programs such as the Department of Health and Human Services, Division
of Public and Behavioral Health, Behavioral Health and Wellness Program and groups such as the Perinatal
Health Initiative should develop a focused campaign and dedicate funding for methamphetamine use in
pregnancy reduction (Level: Facility) (Mentioned twice)
3. Nevada State Medicaid should expand medical appointment transportation access, access to a
community health worker to include community-based settings in addition to medical ones, access to
evidence-based home visitation programs, and peer support counseling through reimbursement for
services by July 1, 2026, and legislative appropriation funds should be given to Medicaid to support
expanded coverage. (Impact: Giant)
4. Nevada State Medicaid should provide acceptable and timely transportation for healthcare needs for
Medicaid recipients by July 1, 2024, with the Division of Health Care Financing and Policy assessing
current system adequacy. (Impact: Giant)
5. Relevant State of Nevada agencies and programs such as the Nevada Department of Health and Human
Services, Division of Public and Behavioral Health Maternal, Child and Adolescent Health, Women Infants
Children and Behavioral Health and Wellness programs should ensure adequate resources related to
physical and mental wellbeing, especially during pregnancy, are given to underserved individuals through
focused outreach to perinatal populations by December 31, 2023. (Impact: Giant)
6. State of Nevada agencies and programs such as the Department of Health and Human Services, Division
of Public and Behavioral Health, Behavioral Health and Wellness Program and groups such as the Perinatal
Health Initiative should address methamphetamine use and treatment and enable providers, including
but not limited to perinatal providers, to refer patients for treatment by providing supportive resources to
enable referrals as well as increase state capacity for behavioral health treatment by increasing total
number of treatment beds by July 1, 2024. (Impact: Giant)

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 46
7. Nevada law enforcement agencies statewide should review law enforcement protocols for domestic
violence offenders to ensure perinatal survivors of domestic/interpersonal violence have protections in
place to prevent death by homicide by December 31, 2024. (Impact: Giant)
8. Insurers and hospitals should provide or reimburse for perinatal patients a medical or behavioral health
advocate, as appropriate, utilizing data collected regarding the different social determinants of health
(SDOH) from universal screenings for SDOH and medical needs, with Medicaid completing an analysis of
possible benefits of perinatal medical or behavioral health peer advocate role coverage by July 1, 2024,
and receive funding, including but not limited to legislative appropriations to expand to cover this
provider type be considered. (Level: System)
9. Nevada Medicaid and wider health systems should provide an avenue for under and uninsured individuals
to access medical care and legislative appropriation funding be provided to allow for Medicaid to expand
services and increase income limits to serve more Nevadans by July 1, 2025. (Level: System)
10. Nevada law enforcement agencies and associations statewide should review current protocol on
supervising parole to ensure perinatal survivors of domestic/interpersonal violence have protections in
place to prevent death by homicide by December 31, 2024. (Impact: Medium)
11. State of Nevada agencies and programs such as the Nevada Department of Education and Department of
Health and Human Services should develop and implement at least two robust evidence-based education-
based programs and support to effectively screen for and address ACEs in educational settings by
December 31, 2024. (Level: System)
12. Relevant State of Nevada agencies and programs should mandate priority access to mental health and
medication assisted substance use treatment for pregnant women by July 1, 2025. (Mentioned two times)
(Level: System)
13. State of Nevada agencies and programs, such as the Division of Child and Family Services, Department of
Education, Nevada Part C and Early Intervention Services programs should develop and implement early
childhood intervention and trauma therapy for impacted children by July 1, 2024. (Level: System)
14. Remove the barriers to accessing mental health care and substance use treatment (Level: System)
15. State general funding should be appropriated to support Medicaid reimbursement for doulas to also
include full-spectrum doulas by July 1,2024. (Level: System)
Extra Large Impact Recommendations
1. Nevada state general funds should be awarded to increase available funding for workforce and pipeline
development programs to mental health providers by July 1, 2026. (Level: System)
2. Prenatal care providers should utilize Final Recommendation Statement: Aspirin Use to Prevent
Preeclampsia and Related Morbidity and Mortality: Preventive Medication | United States Preventive
Services Taskforce (uspreventiveservicestaskforce.org) protocol for prescribing low does 81mg aspirin to
decrease the chance of developing severe preeclampsia and eclampsia and educational campaigns be
developed by local medical professional chapters and the Nevada Primary Care Office to increase
awareness by July 1, 2023. (Level: Provider)
3. By July 1, 2024, State of Nevada agencies and programs such as the Department of Health and Human
Services, Division of Public and Behavioral Health, Behavioral Health and Wellness Program and groups
such as the Perinatal Health Initiative should assess the system for accessing care for people who use
substances in pregnancy and reduce stigma in accessing care given Nevada data show people who use
substances experience delays in accessing care. (Level: System)
4. The State of Nevada, Division of Public and Behavioral Health and Nevada Hospital Association and
Nevada Rural Hospital Partnership should oversee a maternal perinatal regionalization program that
includes emergency maternal transport standardized protocols, by July 1, 2025. (Level: System)
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 47
5. Insurers and birthing facilities should increase access to patient navigators to follow up for up to 1 year
postpartum for high-risk patients, especially those with a history of chronic diseases. By July 1, 2024, State
of Nevada agencies such as the Division of Health Care Financing and Policy should audit Medicaid
perinatal patient navigators and case managers to ensure quality care coordination, timely referral to
needed services, and patient connection to services is occurring. (Level: System)
6. State Medicaid (Division of Health Care Financing and Policy) should receive funding, including but not
limited to legislative appropriations to expand postpartum coverage in Nevada to 12 months to allow
access to behavioral health care and medical care by July 1, 2024. Medicaid policy and reimbursement
changes for behavioral health care treatment to be allowed and incentivized to encourage it to be
performed within medical offices with equal Medicaid reimbursement for medical and behavioral health
services by the end of 2024. (Level: System)
Large Impact Recommendations
1. Hospitals should institute the Alliance for Innovation on Maternal Health Hemorrhage bundle, through
the Nevada Division of Public and Behavioral Health, Maternal, Child, and Adolescent Health Section, to
ensure consistent and accurate risk identification and treatment, by 2024. (Level: Facility)
2. In the event of an obstetric hemorrhage in a facility that does not have an available OBGYN, the hospital
should have a protocol for rapid transport or calling in the OBGYN on call. Protocol should be in place by
July 1, 2024 and could be included in Health Care Quality and Compliance certification and licensing
processes. (Level: Facility)
3. Hospitals, specifically the emergency department (ED) and labor and delivery, should review their facility’s
blood banking practices, and have a protocol in place when there is a lack of available of product. Protocol
should be in place by July 1, 2024, and verifying protocol exists could be included in Health Care Quality
and Compliance certification and licensing processes. (Level: Facility)
4. Institutions and hospitals should standardize response and reporting of abnormal perinatal vital signs and
presence of protocols to do so be part of licensing and certification processes for Health Care Quality and
Compliance, Division of Public and Behavioral Health by July 1, 2024. (Level: Facility)
5. Institutions and hospitals should standardize response and reporting of severe pain to include not only
pain treatment but prompt evaluation of the cause of acute pain and presence of protocols to do so be
part of licensing and certification processes for Health Care Quality and Compliance, Division of Public and
Behavioral Health by July 1, 2024. (Level: Facility)
6. The State of Nevada, Division of Public and Behavioral Health, Health Care Quality and Compliance and
Maternal Child and Adolescent Health and Nevada Hospital Association and Nevada Rural Hospital
Partnership should institute maternal levels of care in healthcare facilities to identify minimal resources to
do obstetric care, by July 1, 2025. (Level: System)
7. The State of Nevada, Office of Primary Care, should increase access to primary care, especially for
geographically remote areas, through the J-1 Visa program and other efforts related to highly medically
underserved areas in the state, including designated maternal health professional shortage areas, by July
1, 2025. (Level: System)
8. For providers, including perinatal medical providers, increase education, buprenorphine training,
universal screening, payment for treatment and collaborative care codes, and payment for integration of
behavioral health within routine practices from Nevada Medicaid; encourage suboxone training in
residency program for OBGYNS and Family Practice physicians and ensure Nevada Medicaid and the
Division of Public and Behavioral Health Behavioral Health and Wellness Program, State Opioid Response
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 48
related committees Maternal Adolescent and Child Health Program, and Perinatal Health Initiative
provide and distribute resources to support and grow these efforts by July 1, 2024. (Level: System)
9. Nevada State Medicaid (Division of Health Care Financing and Policy) should improve availability and use
of perinatal case coordinators and improve patient communication, including legislative allocation of
State General Funds dedicated to expanding existing programs or create new ones to improve perinatal
health outcomes by December 31, 2024. (Level: System)
10. Education by state medical professional associations by July 1, 2024, to prevent failure to recognize the
impact of obesity as a risk factor for poor perinatal outcomes. (Level: System)
11. Provide better continuity of care for people with mental health conditions. State agencies such as
Medicaid should explore other non-tradition ways to engage the health care system including utilizing
home-based nursing care visits and/or telehealth for perinatal patients by July 1. 2024. (Level: System)
(mentioned two times)
12. Increase state general funded programs to improve access to medication assisted treatment for drug
addiction by July 1, 2024 (Level: Community)
13. Nevada State Medicaid (Division of Health Care Financing and Policy) should receive funding including, but
not limited to legislative appropriations to expand postpartum coverage in Nevada to 12 months by July 1,
2024 (Level: System) (Mentioned two times)
Medium Impact Recommendations
1. Providers should create a protocol for staff to follow outlining resources and how to provide a social
services consult to patients, assessing social determinants of health such as housing, employment status,
access to transportation and how it impacts an individual’s health, Nevada Division of Public and
Behavioral Health, Maternal and Child Health program should provide a provider focused social media
campaign to increase use and awareness of the Nevada medical home portal as a resource by July 1,
2024. (Level: Patient/Family)
2. Providers should create a protocol for staff to follow outlining resources and how to provide a social
services consult to patients, assessing social determinants of health such as housing, employment status,
access to transportation and how it impacts an individual’s health, Nevada Division of Public and
Behavioral Health, Maternal and Child Health Program should provide a provider focused social media
campaign to increase use and awareness of the Nevada medical home portal as a resource by July 1,
2024. (Level: patient/family and provider) (Mentioned twice)
3. Providers should use behavioral health techniques and screening tools to help patients come to decisions
to get themselves treatment and Nevada Department of Health and Human Services should consider
developing educational materials and supports for provider education by July 1, 2024. (Level: Provider)
(Mentioned three times)
4. Hospitals should develop an evidence-based protocol and Division of Public and Behavioral Health, Health
Care Quality and Compliance Office should monitor existence of such protocols as part of standard
certification and licensing processes by July 1, 2024, for intravenous fluids iron to treat anemia in
pregnancy, by 2024. (Level: Facility)
5. State of Nevada agencies and programs such as the Division of Public and Behavioral Health should
develop an education campaign on how anemia contributes to maternal mortality by July 1, 2024, and
local medical professional chapters should educate providers on the need to address anemia immediately
when recognized and ensure effective treatment to include IV iron by July 1, 2023. (Level: Facility)
6. State of Nevada agencies and programs such as the Division of Public and Behavioral, Health Care Quality
and Compliance, should ensure hospital Emergency Departments provide a standard prenatal care
workup to patients who indicate they have not had prenatal care when seeking prenatal care by July 1,
2025. (Level: System)
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 49
7. Nevada Systems of Higher Education and private obstetric education programs should include a
psychiatry rotation by July 1,2025. (Level: System)
8. Trauma informed care techniques should be required by relevant boards and certification agencies as a
standard of practice when providing substance use treatment, by July 1, 2024, as well as by the State of
Nevada, Division of Child and Family Services and local child welfare entities in child protection service
provision. (Level: System)
9. Nevada State Medicaid should educate Nevada providers about covered Medicaid services to support
physical and mental wellbeing, by July 1, 2024. (Level: System)
10. Preconception counseling would have been helpful to explain to the patient the risks of pregnancy with
diabetes and chronic hypertension so state agencies such as Medicaid and the Division of Public and
Behavioral Health, community-based organizations, and Nevada medical professional societies should
provide education on this topic regularly to increase awareness and access to family planning by July 1,
2024. (Level: System)
11. Medicaid, Tricare, and private medical insurance should reimburse for interventions designed to help
patients make healthy choices such as going to the recommended number of prenatal and postpartum
care visits as defined by American College of Obstetricians and Gynecologists including, but not limited to,
value-based payments and patient incentives such as diapering supplies by December 31, 2024. ((Level:
System)
12. Medicaid policy to ensure equal payment reimbursement for telehealth as in-person visits by July 1, 2024.
(Level: Community)
Small Impact Recommendations
1. Providers should create a protocol for referring to supportive counseling and education for those patients
who are struggling with adherence to their medical plan and medication compliance, with education and
supports possibly provided by local professional medical association chapters by July 1, 2024. (Level:
Provider)
2. Providers from different fields of specialization should work as a team and communicate when co-
managing disease in a perinatal patient with possible Grand Rounds or Project ECHO supports to facilitate
pathways to support collaboration and identify reimbursement of other barriers to doing so by July 1,
2024. (Level: Provider)
3. Prenatal care providers, including OBGYN’s, midwives, and doulas, should discuss with patients, the
amount and pace of gestational weight gain and nutrition and physical activity in pregnancy. Providers
should develop a protocol for referring patients to a dietician when weight gain exceeds the expected
amount, with provider key resource guide support materials shared by local chapters of professional
organizations by July 1, 2024. (Level: Provider)
4. Providers should be provided education and resources by local medical professional organization
chapters to refer for inpatient treatment when presenting with signs of mania and continued substance
use by July 1, 2023. (Level: Provider)
5. All providers should provide preconception counseling for people living with chronic disease. Community
based organizations and the State of Nevada, Maternal, Child, and Adolescent Health Section, should
develop materials to educate the public about the importance of preconception counseling, by December
31, 2024. (Level: System)
6. State of Nevada agencies and programs such as the Maternal, Child, and Adolescent Health and Women,
Infants, and Children (WIC) Sections and Division of Welfare and Supportive Services childcare and TANF
programs should provide outreach promoting prenatal care, especially in underserved populations, by
July 1, 2023. (Level: System)

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 50
7. The following should be codified in all Nevada medical examiner (ME) protocols that MEs should either
directly examine histologically the conduction system of the heath or consult a cardiac pathologist for
examination of the heart in cases in which cardiac dysrhythmia/arrythmia is the putative immediate cause
of death. Genetic screening for inherited cardiac arrythmia syndromes should also be done, if feasible.
(Level: System)
8. Nevada Peace Officers Standards and Training module for law enforcement should be developed and
implemented by July 1, 2024, to include required evidence-based training to recognize substance use
signs and to ensure appropriate medical monitoring for drug withdrawal following intake into custody
with clear protocols to access timely and medically appropriate treatment. (Level: System)
General MMRC Member MM/SMM Recommendations and
Prevention
1. Work in cooperation with Nevada’s Native American Tribes to identify strategies to address the disparity
in pregnancy-related death among women categorized as American Indian Alaskan Native.
2. The pregnancy associated death ratio is 50% higher in the rest of the state than in Clark County, and more
than triple the ratio in Washoe County. Given this geographic disparity, it may be wise to adopt a formal
perinatal regionalization program that includes identification of levels of care, a system of transfer of care,
and designating emergency transport agreements for mother and child.
Advisory Committee of the Office of Minority Health and Equity
Recommendations
Per NRS 442.767, this report is done in collaboration with the Advisory Committee of the Office of Minority Health
and Equity and the MMRC. Three presentations were made by MMRC staff to the Advisory Committee to share
data and information on MM and SMM and to solicit Committee Member expertise and recommendations to
prevent MM and SMM and to provide any policy or legislative recommendations. Below are the specific
recommendations and feedback from the Advisory Committee after having shared the data presented in this
report and asking for their expertise and recommendations for the prevention of MM and SMM and elimination
of associated disparities evident in the data.
The Advisory Committee seconded the MMRC’s recommendation on providing more accessible transportation for
patients to get to their medical appointments and added that it is key to provide transportation to get from home
to the medical appointment and back. The Advisory Committee noted a lack of transportation is different from a
patient’s non-adherence to their medical plan. The Advisory Committee recommended in-home doctor’s visits or
telehealth options in addition to the need for transportation and noted transportation issues in rural counties
would need a different transportation plan than urban counties. The Advisory Committee seconded the MMRC’s
recommendation for the Nevada Systems of Higher Education and private obstetric education programs should
include a psychiatry rotation. Lastly, an Advisory Committee Member noted the importance of recognizing that in
Nevada, an estimated 40% of OBGYN’s and Family Practice providers will retire in the next 5 to 10 years and
Nevada may see a significant increase in the current shortage of providers.

Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 51
Advisory Committee of the Office of Minority Health and Equity
Members
Chair
Samuel J. Hickson, Ph.D., LMSW, MSSA, MBA, ACE-CHC
Social Worker, Intermountain Healthcare
Vice Chair
Rutu Ezhuthachan MD, MMM, FAAP
Chief Medical Officer, Health Plan of Nevada Medicaid
Medical Director of Quality Improvement, Health Plan of Nevada (UnitedHealthcare Nevada)
Members
Erik Jimenez
Senior Policy Director, Office of the Nevada State Treasurer
Andrea Gregg
Executive Director, High Sierra Area Health Education Center
Rev. Dr. Karen Anderson
Senior Pastor, First AME Church Las Vegas
Dr. Crystal Lee, Ph.D.
Assistant Professor, University of New Mexico, College of Population Health
CEO, Indigenous Health
Reimund Serafica, Ph.D., MSN, APRN, PMHNP-BC, CNE
Associate Professor, School of Nursing, University of Nevada—Las Vegas President, Asian American/ Pacific
Islander Nurses Association of Nevada
Senator Patricia Spearman
Legislator Appointed by the Legislative Commission
Maternal Mortality Review Committee Members
Chair
Sandra Koch, MD, FACOG
Carson Medical Group, Carson City, NV
Members (Current and Past)
Brian Iriye, MD, MFM, Emeritus
High Risk Pregnancy Center, Las Vegas, NV
David Jackson, MD, MFM, FACOG
High Risk Pregnancy Center, Las Vegas, NV
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 52
Erika Washington
Executive Director Make It Work Nevada, Las Vegas, NV
James Alexander, MD, MFM
University of Nevada, Reno, School of Medicine
Jennifer Vanderlaan, PhD, MPH, APRN, CNM, FNP
University of Nevada, Las Vegas School of Nursing
Jollina Simpson, IBCLC, Emeritus
Executive Director, Kijiji Sisterhood
Joseph Adashek, MD, FACOG
Summerlin Hospital and Medical Center, Las Vegas, NV
Laura Knight, MD
Washoe County Regional Medical Examiner’s Office, Washoe County
Melanie Rhee, LCSW
Community Crisis Response Social Worker and Clinical Supervisor
Melinda Hoskins, MS, RN, CNM, IBCLC
Humboldt General Hospital, Women’s Health Center
Natalie Nicholson, DNP, MBA, RN, CENP
Formerly of Women Services, Renown Regional, Reno, NV
MMRC Support Staff and Other Acknowledgements
The Nevada MMRC functions with support of staff from the DPBH, Maternal, Child and Adolescent Health Section.
A special thanks to Robyn Cunnally, Registered Nurse, Taliman Afroz, PhD, MS, Aisha Bowen, MSW, and Cortnee
Scurry, MSW. Ghasi Phillips-Bell, ScD, CDC, provided appreciated support related to summarizing certain key
points. Office of Analytics MMRC support is crucial and deeply appreciated.
The MMRC gives a special thanks to Nicole Reilly and the Nevada Committee on Domestic Violence Fatality
Review for their efforts in joint case reviews. Additional thanks are given to Tegan Callahan, MPH, from the CDC,
Misty Vaughan Allen, Suicide Prevention Coordinator, Nevada Office of Suicide Prevention, Stephanie Herrera and
Freq Quihuis, Office of Vital Records, and Dr. Cornelia Graves for their guidance, expertise, and support.
DPBH would like to thank all members of the MMRC and Advisory Committee, support staff, and local and federal
partners. The members of both committees volunteer their time and expertise and are passionate about minority
health issues and committed to eliminating health disparities.
The families who shared information in informant interviews are deeply appreciated for their generosity in
sharing crucial information in the hopes of preventing other families from experiencing a similar, devastating loss.
We dedicate this report to the memories of all the individuals lost to maternal mortality and to their loved ones.
Supported by the following grants in the Nevada Division of Public and Behavioral Health
State System Development Initiative: H18MC00032
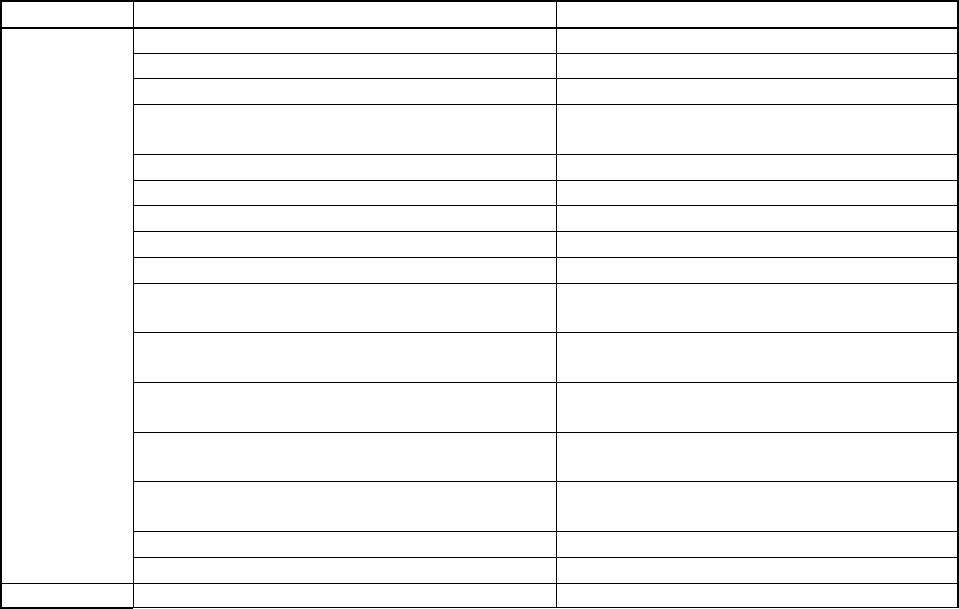
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 53
Enhancing Reviews and Surveillance to Eliminate Maternal Mortality: NU58DP006937
Title V Maternal and Child Health Block Grant: 6-BO4MC45229
Nevada's Initiative to Address COVID-19 Health Disparities to High Risk and Medically Under-served Populations:
NH75OT000092
Appendix
Complete List of SMM Indicators and Associated ICD‐10‐CM Codes
Classification
Severe Maternal Morbidity Indicator
ICD‐10/Procedure Codes
Diagnosis
Acute myocardial infarction
121.xx, 122.x
Aneurysm
171.xx, 179.0
Acute renal failure
N17.x, O90.4
Adult respiratory distress syndrome
J80, J95.1, J95.2, J95.3, J95.82x, J96.0x,
J96.2x, R09.2
Amniotic fluid embolism
O88.1x
Cardiac arrest/ventricular fibrillation
I46.x, I49.0x
Disseminated intravascular coagulation
D65, D68.8, D68.9, O72.3
Eclampsia
O15.x
Heart failure/arrest during surgery or procedure
I97.12x, I97.13x, I97.710, I97.711
Puerperal cerebrovascular disorders
I60.xx‐I68.xx, O22.51, O22.52, O22.53,
I97.81x, I97.82x, O873
Pulmonary edema/Acute heart failure
J81.0, I50.1, I50.20, I50.21, I50.23, I50.30,
I50.31, I50.33, I50.40, I50.41, I50.43, I50.9
Severe anesthesia complications
O74.0, O74.1, O74.2, O74.3, O89.0x, O89.1,
O89.2
Sepsis
O85, O86.04, T80.211A, T81.4XXA, R65.20,
A40.x, A41.x, A32.7
Shock
O75.1, R57.x, R65.21, T78.2XXA, T88.2XXA,
T88.6 XXA, T81.10XA, T81.11XA, T81.19XA
Sickle cell disease with crisis
D57.0x, D57.21x, D57.41x, D57.81x
Air and thrombotic embolism
I26.x, O88.0x, O88.2x, O88.3x, O88.8x
Conversion of cardiac rhythm
5A2204Z, 5A12012
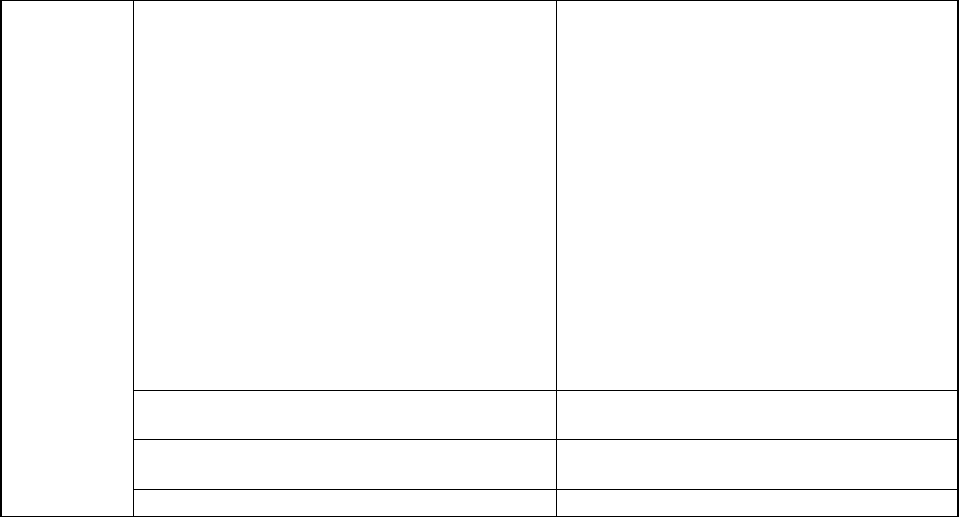
Maternal Mortality and Severe Maternal Morbidity Report, Nevada 2020-2021 54
Procedure
Blood transfusion
30230H0, 30230K0, 30230L0, 30230M0,
30230N0, 30230P0, 30230R0, 30230T0,
30230H1, 30230K1, 30230L1, 30230M1,
30230N1, 30230P1, 30230R1, 30230T1,
30233H0, 30233K0, 30233L0, 30233M0,
30233N0, 30233P0, 30233R0, 30233T0,
30233H1, 30233K1, 30233L1, 30233M1,
30233N1, 30233P1, 30233R1, 30233T1,
30240H0, 30240K0, 30240L0, 30240M0,
30240N0, 30240P0, 30240R0, 30240T0,
30240H1, 30240K1, 30240L1, 30240M1,
30240N1, 30240P1, 30240R1, 30240T1,
30243H0, 30243K0, 30243L0, 30243M0,
30243N0, 30243P0, 30243R0, 30243T0,
30243H1, 30243K1, 30243L1, 30243M1,
30243N1, 30243P1, 30243R1, 30243T1
Hysterectomy
0UT90ZZ, 0UT94ZZ, 0UT97ZZ, 0UT98ZZ,
0UT9FZZ, 0UT90ZL
Temporary tracheostomy
0B110Z4, 0B110F4, 0B113Z4, 0B113F4,
0B114Z4, 0B114F4
Ventilation
5A1935Z, 5A1945Z, 5A1955Z
